
Stopping Gout Together › Forums › Help My Gout! The Gout Forum › Febuxostat dose change. Or different time of day?
Tagged: Adenuric/Febuxostat/Uloric Forum Topics, Forum for Gout Patients, Uric Acid Control, Xanthine and Gout Forum
- This topic has 40 replies, 3 voices, and was last updated 3 years, 9 months ago by
d q.
-
AuthorPosts
-
-
October 9, 2018 at 10:24 pm #8086
d q
Participant
Firstly, where you been nobody? You seem to have gone awol..? 🙂
Ok I finally have all the results in and wanted your opinions;
18th April – 388 ummol (60mgs)
23rd May – 413 ummol (80mgs) <— Strange result
18th June – 377 ummol (80mgs)
11th July – 360 ummol (80mgs)
15th August – 346 ummol (80mgs)
24th September – 350 ummol (80mgs)
3rd October – 362 ummol (80mgs)So doing the most basic of maths (377+360+346+350+362 / 5) = 359 ummol.
Best result being 346 and the worst at 377.
It looks like the Febuxostat is maxing out at no lower then 346 ummol.
I doubt more blood tests will change figures significantly so I guess I’m at the cross roads. Do I move up to 120mgs? Or try 100mgs? or Stick with 80mgs?
(Liver markers all seems OK so far).Can sticking with 80mgs cut it as more crystals dissolve in the hope that the overall UA levels drop further cementing 80mgs or is it too risky?
Thanks guys!
p.s. @nobody – come on show yourself! The forum can get lonely without you! 🙂

Gout Pills Before, During, or After Food?
-
October 9, 2018 at 10:38 pm #8087
nobody
ParticipantMy opinions and Keith’s differ in some respects so I thought it best to let you discuss your issues with him since he was (unusually?) available.
Seeing that your new blood medication doesn’t seem to do anything, yeah: the obvious thing to do would be to increase your febuxostat dose. In my opinion, your should try around 100mg (precision doesn’t matter) rather than 120mg to begin with. 80mg would probably be enough in the long run but a higher dose might help you bet better faster so as long as there are no obvious side effects, a moderate dose increase seems worth trying.
We had discussed all of this earlier but if it encourages you to see me restate it, it only takes a few minutes so here you are.-
October 12, 2018 at 7:43 am #8109
 Keith TaylorParticipant
Keith TaylorParticipantThanks, Nobody.
I like to think that our experiences differ. So some of our conclusions and opinions might be different. But we both seem to share a passion for helping people with gout problems. So I hope that continues for a very long time.
Ultimately, if we get gout patients to talk to their doctors with greater clarity on both sides, I think we’ve achieved something good.
I’ll get back on topic in a separate reply.
-
October 13, 2018 at 12:20 pm #8169Participant
Certainly we seem to have had different experiences with doctors, Keith.
Their expertise is obviously vital in some situations and I would sooner trust a NHS doctor than most others but I would still not trust everything the best doctors say because the demands of their jobs take a heavy toll on their ability to reason systematically… assmuming they are even willing which is in my experience generally not the case.The way I see it, your website’s most valuable contribution comes from the effort you invested in selecting and presenting some of the evidence about gout in an accessible manner. Even when I think you’re wrong, your work is typically helpful anyway because you’ve put int the time necessary to reference facts in a fairly unbiased manner.
I’m afraid I don’t have that much patience. And even if I did, the effort would typically be wasted in a web forum post.
-
-
October 11, 2018 at 9:06 pm #8101Participant
My opinions and Keith’s differ in some respects so I thought it best to let you discuss your issues with him since he was (unusually?) available.
Totally true. Besides you know how much I value both your opinions. In most cases I seek no further opinion. You and Keith have been absolutely fantastic during my troubling times even though Keith goes missing sometimes and leaves us to deal with the boards 🙂 and you both continue to be, so thanks mate.Yes, the blood medication seems to have been and continues to be a total waste of time. I think I’ve been dealt the placebo with no way of telling until around May next year which is approximately when the unblinding occurs and if I am on the placebo I’ll finally be given the genuine drug around then too (hopefully). So I guess it’s going to have to be a XOI’s for the foreseeable future.
Yep, I think your advice is spot on, I’ll try 100mgs from next week so to time with my next blood test in about 2 weeks. I really really hope I can return to 80mgs at some point. Just a few questions;
1. How long would a fair trial of 100mgs be before attempting a return to 80mgs?
2. Would another option be alternating between 80mgs on one day and 120mgs the other (or similar)? Otherwise its going to have to be pill cutting again.
3. Would you recommend a tablet of colchicine nightly during the first 2 weeks or so? or have the numbers been low enough for long enough to not really worry too much?
@nobody – Believe me your posts definitely encourage me. 🙂 For that matter I don’t really know where I would be without your sound advice about this subject at times. It’s been a steep steep learning curve with bad bad times.
@Keith – anything to add sir? -
October 11, 2018 at 9:56 pm #8102Participant
How long you would take 100mg should depend on your test results, gouty symptoms and the subjective side effects of the dose increase. We’re potentially talking years but maybe you could try to aim for a slightly lower dose such as 90mg after a while depending on what 100mg does.
I don’t know much about the effects of a large febuxostat dose over the day but based on the little I know, I’d cut rather than alternate. My rheuma agreed on that point but we were discussing much smaller doses. You could also try taking your dose at a different time to see if that makes a material difference by the way (tests have shown the effect is slightly different if you take the pill on an full as opposed to empty stomach).
At this stage, I wouldn’t recommend a daily colchicine dose. If you were to feel incoming gouty symptoms a few days after the dose increase though, you could go for a pill just in case (and quit colchicine once that went away). -
October 11, 2018 at 10:30 pm #8104Participant
Thank you so much for that advice @nobody !
I’ve never ever tried taking it at different times actually or with a full or empty stomach. I presently take it on an empty stomach as soon as I wake up (would that be the most concentrated way? or could I achieve better results taking it after lunch or breakfast for example going by those studies/tests?
Assuming any changes to the above causes a drops in UA by another 10 or 20 to say 330-320 would there still be a case to try 90-100mgs..?
Yea, I thought I would reserve the colchicine for the potentially bad days too.
Thank you so much mate. Thanks
-
October 11, 2018 at 11:07 pm #8105Participant
You apparently get a taller peak but a lower average blood concentration if you take the drug on an empty stomach. So the drug might be more effective if you take it on a full stomach… assuming of course you haven’t eaten something which impairs absorption in the first place. But possibly it might be even more effective to take it at a time of the day when you wouldn’t normally eat (this is a wild guess but taking it in the morning doesn’t sound ideal).
I’m pretty sure none of this would make enough of a difference to warrant postponing your dose increase anyway. It’s just something pretty harmless you could try, like next year or something. If you’re going to have frequent blood tests anyway you could use the opportunity to run some experiments. -
October 12, 2018 at 7:58 am #8110Keith TaylorParticipant
In response to Nobody’s:
At this stage, I wouldn’t recommend a daily colchicine dose. If you were to feel incoming gouty symptoms a few days after the dose increase though, you could go for a pill just in case (and quit colchicine once that went away).
The only gout doctor I ever trusted advised 2 weeks colchicine with each allopurinol dose increase. So because I trusted him that’s exactly what I did the first couple of times. Then I went back to “as-required”.
For me, that worked better. But I’d had many years of recognizing gouty symptoms. So I could know upon waking if a flare-up was imminent. In which case, ibuprofen almost always worked for me.
It’s not that I’ve anything against colchicine. But personally, I found ibuprofen a better choice for me. So I feel it’s very important to:
1. Understand how each different type of gout pain relief works.
2. Be aware of your gout symptoms each and every day.
3. Discuss your options with your doctor so everyone involved is “singing off the same sheet”.In terms of uric acid treatment @d-q have you discussed uricosurics with your doctor in combination with febuxostat? I can’t see anything in your history here, but the search of topic histories is as fallible as my memory. 😉
-
October 12, 2018 at 8:46 am #8116Keith TaylorParticipant
I should have added that if uricosuric combinations are not an option, I agree with:
1. Cutting febuxostat pills to get 100 mg per day. Because alternating between 80 mg and 120 mg seems like too much of “rollercoaster”. If we were talking about allopurinol, I might have a different view. But febuxostat is metabolized differently.2. Time of day, especially in relation to meals is likely to have an effect. Though studies disagree if the action of food is significant or not. But frustratingly I can’t find any real-world studies on gout patients. So it looks like ” If you’re going to have frequent blood tests anyway you could use the opportunity to run some experiments” is a good option. However, you need to be aware that experiments involving a single subject are extremely hard to get convincing results from 🙁
-
October 12, 2018 at 9:19 am #8120Participant
@nobody – Very interesting indeed – thank you so much. Maybe I’ll start taking it after lunch as my next blood test is indeed in two weeks and I can use this as my last attempt to see if 80mgs made a difference or not. I normally have late lunches (2pm-4pm) so would an attempt to take it after then or maybe even dinner at around 9pm be a quick two week trial to run? Or would you consider trying after breakfast (normally two slices of toast, banana and some kiwi with a home made latte)? My only concern being the milk possibly impairing the absorption or is milk fine?
-
October 12, 2018 at 11:16 am #8127Participant
@keith – Thanks for that information. The only time I ever tried colchicine was during an attack I had about a month or so ago. I took the maximum dose and was able to reduce the term to around 3-4 days. During my previous attack I took maximum dose of 500mgs Naproxen twice a day with no real benefit.. It brought relief don’t get me wrong but it didn’t seem to end the gout attack. I believe Naproxen is even stronger Ibuprofen even?
Uricosurics did come up in a few of our consultations however the general advice that was always given was “If we are able to control it with one medication then that would be the safest way – Uricosurics are generally taken twice a day and sometimes come with unwanted side effects” I’m personally not too sure about the dosing or the side effects since the Febuxostat would be there too but I guess if we still have a little more room with Febuxostat shouldn’t we explore that first?
Yep, going by both of your recommendations cutting seems to be the best way however reducing a 120mgs pill to 100mgs or adding a further 20mgs to an 80mgs pill is indeed going to be challenging. My pill cutter only cuts pills in half so its going to have to be either a knife to the 120mgs or 80mgs cut twice in addition to a full tablet! There’s going to be a few bits here and there.
The time of day situation is very interesting and I’ve never attempted to test it so since I have a blood test in about two weeks I’ve decided to give it one last shot. The question is when would be the best time to take it and what hinders its absorption. I know this can get very technical but in general how could one modify their schedule to potentially see the best or any benefit. @Keith I know you take Allopurinol so things might be a little different but time of day? @nobody I know our doses are oceans apart but with what and when do you normally take your dose?
If there wasn’t enough questions above already what UA level should one be targetting now. I know Keith loves the lower the better approach but what is considered adequate since I’m coming to the maximum dose?
Thank you both so much. Means a lot really.
-
October 13, 2018 at 10:56 am #8141Keith TaylorParticipant
100mg Febuxostat
I think you might approach your pharmacist with the 100 mg febuxostat problem. Because some offer pill-splitting as a routine service. But it’s not something I have personal experience with. If your pharmacist does offer this, I suggest halving 80 mg and 120 mg tablets. Then half of each = 100 mg (my days of watching Rachel Riley have not been totally misspent 😀 )
Febuxostat time of day
If you were a mouse, I’d say 2 hours after your keeper turns on the light is the best time of day to take febuxostat. Because that worked well in:
Kanemitsu, Takumi, Yuya Tsurudome, Naoki Kusunose, Masayuki Oda, Naoya Matsunaga, Satoru Koyanagi, and Shigehiro Ohdo. “Periodic variation in bile acids controls circadian changes in uric acid via regulation of xanthine oxidase by the orphan nuclear receptor PPARα.” Journal of Biological Chemistry (2017): jbc-M117.we also demonstrated that the antihyperuricemic effect of the XOD inhibitor febuxostat was enhanced by administering it at the time of day before hepatic XOD activity increased. These results suggest an underlying mechanism for the circadian alterations in uric acid production and also underscore the importance of selecting an appropriate time of day for administering XOD inhibitors. […] the excess production of uric acid induces hyperuricemia and gout in humans. XOD inhibitors are often administered to these patients after meals during the daytime. Febuxostat has an apparent elimination half-life of approximately 5 to 8 hours (46); therefore, this drug is generally taken once a day, mainly in the morning. In hyperuricemia model mice, the anti-hyperuricemic effect of febuxostat was enhanced by its administration in the early light phase (ZT2), during which nocturnally active mice begin to fall asleep.
I’m finding it hard to interpret that in human terms. But if it does translate then the right time for humans is before going to sleep. Also that ties in with other claims I’ve read that uric acid rises through the night in humans. Sorry it’s not exact, but that’s the best I can suggest for now.
-
October 13, 2018 at 11:44 am #8168Participant
Good idea about halving both types of tablets! These tablets halve easily under a little finger pressure. No need for a cutting tool.
After one’s last meal of the day might be a good time to take the drug. But if you’re going to experiment, you might as well try different things. We might be surprised by what works best.I have no idea what might impair febuxostat absorption. Trial and error will tell if anyting makes a significant difference.
For my own use I don’t care about the effectiveness of the drug anymore so I’m taking it pretty randomly. The perceived side effects have become milder over time but they’re still my main guide as to when’s the best time to take it.350 umol/l is generally considered low enough but guidelines recommend aiming a bit lower in some cases. Check out the guidelines and studies for yourself if you have any doubt. Thing is, everyone is different and mesurements are unreliable. Experience might tell you should aim lower than is generally recommended. But it’s way too soon to assume your case in unusual.
Keith has shown evidence that large tophi shrink quicker when you go well under 350 umol/l but you can’t generalize that to people who have already dissolved all their superficial crystals and that study also showed diminishing returns after a certain point. So I can’t say I’ve ever seen any evidence supporting his recommendations on aggressive XOI dosing.
It would be a different matter if 300mg allopurinol was enough to drop your SUA under 300 umol/l without apparent side effects for instance. In that case, ir woudn’t be unreasonable to take 300mg instead of 200 even though the latter dose would be sufficient to reach the generally recommended SUA target. But febuxostat is a newer drug and you’re already taking a dose which isn’t as thoroughly tested as the doses originally recommended by the drug’s developper so there is the balance of risks to consider…
You didn’t try the maximum doses for either Naproxen or colchicine by the way. That said, it may not be prudent to take more than you did in your situation. Anti-inflammatories routinely kill their users. -
October 25, 2018 at 5:41 pm #8466Participant
@Keith – thank you for that excellent post / idea!
Hi, I’ve also done some reading and yes 360ummol is generally the cut off line and with 350ummol being the absolute limit. I guess me still being in the treatment stage and not the maintenance phase I would assume a little lower would be more beneficial? Out of curiosity @nobody, what UA levels would you recommend as a safe and stay in zone whilst in the treatment phase prior to going into maintenance levels? <300 or would <330 be fine for a few months?
On another note and I know its being actively discussed in another thread is the possibility of cutting pills. I had a little talk with my pharmacist the other day in regards to splitting the 120mgs and the 80mgs to get 100mgs and she strongly recommended I do not do this. I asked for her reasoning and she said it is treated so that is absorbed further down the gut. Splitting the tablet exposes one side to stomach acids which can disrupt this process. Now we both know I split the tablets from day one all the way to get to 80mgs and things seemed to work fine however I did some internet reading a little later and will post the references when possible but apparently splitting these tablets is indeed not recommended. From what I understood is;
If a tablet is not scored then there is no guarantee of chemical / medicinal distribution, dissolution rates and chemical stability within the tablet according to the FDA and certain other articles. You could get 75% of the 80mgs on the left and 25% of it on the right. That would give you 60mgs if you took the left of the tablet and no more then about 20mgs if you took the right.
Now I’m not too sure of this is to protect drug companies or how much of this is to guarantee people continue to pay for larger doses even though it is not required but it really has got me a little worried with the 50% 120mgs and 50% of 80mgs. Let’s say if all this is true especially the distribution part; wouldn’t that then mean there is a possibility I could get 80mgs from the 120mgs tablet split and 60mgs from the 80mgs split totalling more then 140mgs which even more then 120mgs I am trying to avoid taking?
I’m a little bewildered as to what to do..?
-
October 25, 2018 at 6:12 pm #8467Participant
So here are the links and info @nobody and @Keith;
Against Splitting:
1. Contacted Takeda / Menarini directly who have explained that they cannot guarantee uniform active chemical distribution (Febuxostat) throughout the Adenuric tablet at both available doses in the UK. They said they are aware that medical practitioners do occasionally alter/offer doses in this method (for various different reasons) however this is an off-label approach. I asked her to send me the technical document stating this however she said the document is confidential and for internal use only. She will however; send me an email confirming the above.In Support of Splitting:
1. https://www.nps.org.au/radar/articles/febuxostat-adenuric-for-chronic-symptomatic-gout – [reading this throws out everything Takeda / Menarini told me however it doesn’t mean to say Takeda are incorrect (distribution of Febuxostat in the Adenuric tablet)].2. https://www.sciencedirect.com/science/article/pii/S1319016413001254
3. http://www.gout-pal.com/gout-pal-forum/please-help-my-gout/anyone-cut-uloric-80mg-down-to-40mg/ [Interesting post sometime ago here which @Keith mentions a similar situation]
I know I presently need more of the drug but I don’t know how to safely obtain it without going all the way to 120mgs :/
What a pickle this is indeed!
-
October 25, 2018 at 8:30 pm #8468Participant
First, it would indeed be safer for you to cut a bit off the 120mg pill than to combine two pills. I think the risk is neglibible and I would combine pills if I needed to but I’ve never actually tried it, I of course have no proof it is safe and I understand if you don’t want to take chances…
I have however been splitting a single pill in order to take it over several days for quite some time. And the blood tests have been consistent with the dose being controlled as one would expect by splitting. The test results aren’t subtle or overwhelmed by noise.
However it is conceivable that there are differences from one day to the next between the actual doses I’ve been taking and that these differences cancel out over time. If what mattered most for uric acid as well as the side effects I’ve experienced is how much febuxostat one takes over a week rather than over a single day then of course it wouldn’t matter much if the stuff was poorly distributed through the tablets I’ve been splitting.
Subjectively, I did experience different side effects over the course of a single day from taking half a pill as opposed to a quarter of a pill but these side effects haven’t been as consistent as the test restults and might conceivably have been driven more by the dose I thought I was taking than the dose I was actually taking. That’s kind of a strech since I was initially suprised by the side effects but I can’t rule it out nor can I prove it wrong with objective measurements.
Other potentially deadly side effects might conceivably show up if you were to take more than 120mg over a single day. I have zero experience with this and can’t rule it out either so again, I understand if you don’t want to combine pills.This stuff about non-absorption in the stomach however is laughable considering that they do sell scored tablets which have no film between the scored halves of the pill. There also are ingredient lists on the packages… what do the scored tablets contain that would prevent absorption in the stomach? And the studies backing their marketing authorization in several countries look at the effect of 40mg which you can only get by splitting these tablets. Are we to believe than they spend money on separate manufacturing processes for no other purpose than to harm people who split non-scored tablets?
Please consider you are basically talking to a non-sadistic but murderous psychopath when you’re talking to people representing certain pharmaceutical interests. What they are doing kills people and they are doing it for profit. There are cheaper, less dangerous and more conveninent pills and dosing recommendations in many countries and there is no medical reason we couldn’t use them. But we have to put up with this shit for no other purpose than to create a monopolitic rent. -
October 26, 2018 at 12:01 pm #8475Keith TaylorParticipant
@d-q I spent some time a few days ago looking at pill-splitting. Then, I refrained from posting. Because I found that the bewildering range of opinions and practices was likely to cause more confusion. So welcome to my club for the bewildered.
To clarify some points:
– 40 mg Uloric is manufactured and sold in the USA with FDA approval. It’s also available in its home country of Japan alongside a 20mg dose. But the UK NHS approach is that 80 and 120 are acceptable doses.– Doctors have always had the power to prescribe “off-label”. But that raises the question of how to supply it. In earlier discussions (regarding Colcry$) it has been suggested that compounding pharmacists could fill any off-label prescription to get round manufacturers “monopolitic rent”. At the time, I thought such pharmacies were USA-only. But I just found http://www.bcm-specials.co.uk/ as a UK example. Though I haven’t found if there is a UK compounding pharmacist who will create lower-dose pills.
– I also found a European study comparing 40 mg and 80 mg febuxostat. But they had to split 80 mg pills to get the 40 mg dose. They include the disclaimer in the report. Which is similar to my disclaimer below. So after considering all the data related to splitting or not, you should discuss this with your doctor.*
– During my research I stumbled across professional pharmacy forums which confirmed that pill-splitting is very much a pharmacists personal choice.
– Nobody hit the nail on the head about the coatings. If there was an enteric element, it would have to be listed in the ingredients.
In essence, there is no right or wrong answer to this. So if you always cross at the crossing, do not split pills. But if you save yourself the longer walk because you understand how traffic works, get a decent quality splitter and ignore the
trafficpill wardens.* Flendrie, M., B. van den Bemt, V. Huiskes, M. Hoefnagels, and F. van den Hoogen. “AB1034 The urate-lowering effect of febuxostat 80 mg and 40 mg (80 MG FILM-COATED TABLETS SPLIT IN HALF) in gout patients in daily clinical practice.” (2018): 1633-1633.
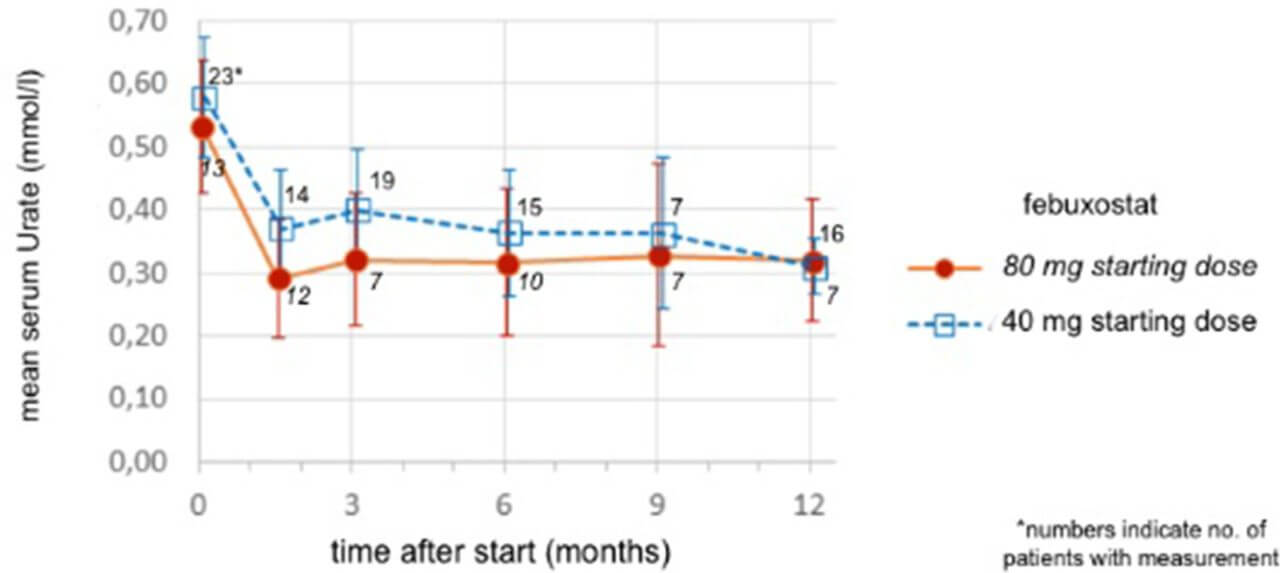
Uloric 80 mg vs 40 mg Uric Acid chart
-
October 26, 2018 at 12:31 pm #8479Keith TaylorParticipant
More on compounding pharmacies in the UK.
Though they can create just about anything, it raises the question: Who will pay for it?
Now, this is governed within the NHS by the Drug Tariff Specials. Which means your doctor can prescribe any dose for drugs on that list, and the NHS will pay for it. For anything else, you will pay.
So now, I have to upset you @d-q. Because liquid allopurinol is on the list. Which is great for micro-titrating to build tolerance in cases of bad side-effects. But no mention of this new-fangled febuxostat stuff 😥
-
-
November 4, 2018 at 1:33 pm #8685Participant
Thank you both for those invaluable responses. I delayed responding until today because I have a small update for you both and would like your advice;
1. I did my usual haematology bloods the other day and UA levels had risen to 408ummol on 80mgs! That’s the highest level I have had since starting 80mgs months ago. Two days prior to the blood test I did take two colchicine tablets as I did have very similar gout pain and didn’t want to risk it. It wasn’t major by far but it was definitely noticeable. Could the elevation of UA levels be something to do with that pain? Maybe a minor gout attack? Maybe just noise?
2. I decided to take on board your advice and f**k it just split both pills in half to get 100mgs. I’m on my 7th day on this dose and so far things seem OK. I’ve got my next blood test in a 3 or so days which I’ll use to check usual markers. I relies it may not be long enough but at least will give pointers.
What I was thinking was I could potentially try 90mgs? Maybe cut the 120mgs into 2 then split that again into 2. So 60mgs + 30mgs? Would that be better then going straight to 100mgs?3. @nobody you mentioned it was about how much you take over the week and not really over how much per day, I was wondering how that would pan out if I took an alternating dose of 120mgs and 80mgs. We discussed with @keith that this is not Allopurinol to have miniscule adjustment leverage but alternating whilst starting on 80mgs gives a total of 680mgs weekly dose whereas 100mgs would give a total of 700mgs. Would alternating really be that much of a problem? Pill splitting is not an issue, it’s just curiosity really as it adds a touch more convenience..? [The possibility of taking over 120mgs a day despite the risk being low is just a little worrying (drug distribution in conversation)]
4. Agree with you both on the coating side of things – I started at 20mgs cutting all the way to 80mgs and saw no real difference in overall results.
5. The commercial side of things applies to everything. Its a cold world and nobody really has anyone’s interests at heart in the medicinal world. Sometimes I even think major sport results are rigged. Which in some cases probably are! I guess you gotta look at the very minor but important plus side which is it provides jobs and security for people.
6. I had a look at that site and indeed it is very interesting. My rheumatologist did discuss with me in the earlier days how I was achieving 20mgs cuts and 40mgs and 60mgs etc. I simply explained I cut the pill twice. He’s first and most immediate reaction was a little grin and then went on to say how are you guaranteeing even distribution of the pill when you do such minor cuts..? I simply responded with, I can’t guarantee it but the bettering results can 🙂 The conversation ended there which suggests he may not be approving of the technique.
Finally, I’m just using a standard pill cutter that I purchased from boots a while ago. Seems to do the trick. Occasionally splits a larger piece but then I take the smaller piece of the other split pill 🙂
and to end on;
Thank you for contacting our company regarding our product, Adenuric (febuxostat).
You enquired if the Adenuric 80mg tablets can be halved to deliver a 40mg dose. As stated in the SmPC (section 4.2): The recommended oral dose of Adenuric is 80 mg once daily without regard to food. If serum uric acid is > 6 mg/dL(357 μmol/L) after 2-4 weeks, ADENURIC 120 mg once daily may be considered. We do not recommend that the 80mg tablets are halved in an attempt to obtain a 40mg dose. Adenuric tablets are not intended to be split, are film-coated and have no score line. In addition, the formulation does not guarantee an even distribution of the active ingredient throughout the tablet. This would constitute an unlicensed use of febuxostat.
We hope this information proves useful to you.
Allopurinol dosing in liquid form* – If only it worked for me ey..
-
November 4, 2018 at 6:12 pm #8686Participant
I don’t think it’s about the weekly dose actually. I merely brought it up as a possibility to question my own conclusions. I go through such mental exercises because like most people, I’m prone to confirmation bias.
Yes, the UA elevation could have something to do with the pain. The elevation could have contributed to the pain or be merely an effect.
I think that going back down to 90mg is a waste of time since you’re already doing 100mg, especially given that disappointing test result.
re: “The commercial side of things applies to everything.”
It’s common for folks in medical research to have altruistic or simply scientific motives. Morally defunct bright people tend to choose more profitable careers. I’d trust developers over those who are only bright enough to profit off the work of others (and in this case, who are so unsrupulous as to call it “our product”).
There are Adenuric tablets featuring a score line out there. But they kept the biggest lie for the punchline: “We hope this information proves useful to you.” -
November 4, 2018 at 11:09 pm #8687Participant
Hi, yea I’ll stick with 100mgs for a little longer and see how that goes. Once I do those bloods in a few days I’ll report back. The convenience of that single 80mgs dose was so ideal – this splitting thing can be cumbersome at times.
Can’t I just split 10 pills and keep them in a pill box!?I know we discussed this but with a sporadic result like 408ummol, could it be a cluster of crystals dissolved and is what raised the UA levels? The reason I am asking is the blood test was taken literally 48 hours later and the only TWO thing occurred/changed prior;
1. I changed to taking Febuxostat with food rather then without. Maybe the amount of medication absorbed is slightly less? (Which I have stopped BTW).
2. The ‘possibility’ of a gout attack two days prior to the blood test (although that would reduce numbers slightly wouldn’t it?)
Cheers.
p.s. Just out of curiosity would another way of playing this be taking 120mgs for a few months and then roll back to 80mgs..? (Lower results –> quicker return to lower dose approach)?
re, re:
“We hope this information proves useful to you” – do me a favour, all bu***t. -
November 4, 2018 at 11:50 pm #8688Participant
Your guesses are as good as mine.
-
November 5, 2018 at 11:17 am #8690
-
November 5, 2018 at 4:49 pm #8692Participant
I have trouble making sense of the stars in your words.
I really think the guesses you’ve taken in your previous post were sensible. But your guesses may turn out to be wrong, same as mine. What more is there to tell?
Besides what I already told you ealier, I mean (like: doses above 80mg aren’t very well tested so I wouldn’t rush into 120mg no matter what dishonest people claim about the safety of that dose).OK, now that I have a bit more time there’s one thing I see I could add: an attack might raise your SUA as well as lower it. My guess is that attacks tend to raise your SUA when it’s low thourgh dissolution and lower it when it’s high through antibody-driven precipitation (your SUA on 80mg febuxostat or more would in this context of course be considered low).
I should also add: blood tests vary randomly. Yes, getting the results you’ve gotten through purely random variations isn’t very likely. But random variations don’t have to be pure. You’d need more than one elevated result in the same circumstance before you could claim (even tentatively) to have grounds on which to explain away such outliers. Were the circumstances of your May test similar in any way?
-
-
November 11, 2018 at 10:06 pm #8737Participant
I have trouble making sense of the stars in your words.
So;T**t – twkrit..? (After literally searching for an hour I can’t find the name you once told me I had the honour of using! so remind me again!?) [Post#8690]
bu***t – bullshit [post#8687] 🙂
Apologies for the delay – a few close relative problems have kept me away from the internet for a while.
Thank you so much for making the effort and that last post mate. I know I can sometimes be a little frustrated and repeat questions but I guess it’s all part of the learning curve and even recovery curve. The rise and drop of SUA explanation you gave really helped me get my head around a few things. You highlighted an extremely important point which was indeed my May results too which were completely paradoxical yet stabilised shortly afterwards. I’ve been on 100mgs for around two weeks and my next blood test is in about 10 days.
The last 18 months have been so tough – thank you so much for your support @nobody and @keith.
-
November 11, 2018 at 11:42 pm #8738Participant
@nobody – actually, something I wanted to ask you. Do you watch the ph value on the water you drink? Should one be watching this as the most recent delivery was a ph value of 6.7 which is slightly acidic, etc.
Cheers buddy
-
November 13, 2018 at 11:42 am #8741Keith TaylorParticipant
Probably best to start a separate topic on Alkaline Water. But the main points are:
1. Don’t paper over the cracks of a bad diet by supplementing with chemicals.
2. The pH of what goes in is irrelevant (except for certain types of reflux disease). It’s the pH of what comes out that matters.
-
-
November 12, 2018 at 7:44 pm #8739Participant
I don’t know anything about what the pH of water would do. I don’t watch it and my assuption is that the food you eat is what matters most (extreme situations excepted). And I don’t think it’s the pH as such which matters. But possibly my assumptions are wrong. In priciple, I don’t see why you couldn’t put enough minerals in water to make a difference.
It’s tawrikt. Or Tauriqt. The spelling is irrelevant. You’re not supposed to write it on stuff anyway. On the contrary, free men write on it.
-
November 13, 2018 at 11:35 am #8740Keith TaylorParticipant
It’s tawrikt. Or Tauriqt. The spelling is irrelevant. You’re not supposed to write it on stuff anyway. On the contrary, free men write on it.
Oui! 🙂
But this man struggles to hold pen to paper after decades of keyboard use. So maybe I’m not as free as I thought I was.
-
-
November 13, 2018 at 12:07 pm #8742Keith TaylorParticipant
To get back to your uric acid test results fluctuations @d-q
I can understand your “need to know reasons”. In fact, it’s one of the cornerstones of an article I’m researching about doctor-patient relationships in gout management.
But I’m sorry that I can’t really add to the points already discussed. Except to think that the most likely explanation is that clusters of uric acid crystals dissolve haphazardly. So no uric acid blood test can accurately measure the debulking process. Ironically, they only become “accurate” in this context once the debulking phase has ended. So without DECT, there’s no way of knowing.
Sorry, I can’t give comfort. But the best analyst of individual results has to be the doctor who ordered the test. I trust you voiced your concerns about your results. So what response did you get?
I think doctor’s answers are very important in gout management. Because when I was at a similar stage to you, I was extremely frustrated that I knew more about uric acid test results than 3/4 doctors I consulted. Happily, the last one gave me all the help and support I needed. I still remember how I felt as if I was walking on air when I strolled home after that consultation.
Our medical situations are different @d-q. But the strength of good doctor support is something that helps all gout sufferers.
-
November 22, 2018 at 2:33 pm #8765Participant
Hi @Keith – Yes, truth be told the frustration I’m going through and still enduring with rheumatologists that don’t really understand gout as much as I thought they would makes me sick. I’m constantly battling them with the most simple of questions yet their answers are jotty at best. Simple examples;
Me: “But we need to get lower then 413ummol for safety?” (May consultation)
Doc 1: “Not necessary, its normal now so just continue as usual”Me: “Don’t we need to monitor liver and kidney whilst on this drug”
Doc 2: “Yes, we can do those tests too”Me: “Shouldn’t we start with a lower dose first (80mgs Febuxostat)”
Doc 2: “It’s fine go for 80mgs straight away”Me: “Shouldn’t we do a 24hr UA test” – this went on for over around a year
Doc 1 and 2: “No need, it wont change treatment options” – Possibly true I guess…——————————————————————————-
This DECT scan is what I want to ask about next but I get this pessimistic feeling he wont do it (or know what it is).
@Keith – I’ll start another topic on the Alkaline Water side of things.
@nobody and Keith – On the other side of things; the blood test result after moving to 100mgs now stand at 340ummol. So it seems that extra 20mgs dropped us +-20ummol and that previous 413ummol does like you say show some sort of artefact. Definitely diminishing results in respect to what 20mgs initially done for me back when I started however it’s still an improvement.I have another blood test coming up in a week or so for my hemo which will include urate so we can see what that result shows although it will only be a 9 day gap from the previous test.
If it still lies within ~340ummol would you recommend going up to 120mgs?
I know 350ummol and below is “good” but not “safe” according to Keith’s chart and i’m a little bewildered as what to do going forward? :/Thank you both so much!
-
November 22, 2018 at 3:06 pm #8766Participant
Quick Reference:
18th April – 388 ummol (60mgs)
23rd May – 413 ummol (80mgs) <— Strange result
18th June – 377 ummol (80mgs)
11th July – 360 ummol (80mgs)
15th August – 346 ummol (80mgs)
24th September – 350 ummol (80mgs)
3rd October – 362 ummol (80mgs)
29th October – 408 ummol (80mgs) <— Strange result possibly artefact
19th November – 340 ummol (100mgs) <— Lowest result but very diminishing returnGoing by the 15th August and 24 September results its a very slight decrease 🙁
-
November 22, 2018 at 8:52 pm #8767Participant
See how long you stuck to 80mg before increasing your dose? It’s obviously too soon to think about increasing it further.
340 is only one result. You don’t know how your average on 100mg will look like. Comparing it to your 346 result is wrong. That was the lowest out of 7 results! Your average on 80mg has been 374.
And you should be monitored for sides effects for a while. 100mg is an uncommonly strong dose so make sure everything is being checked (for instance: not just ALT and AST but ALP as well). Mind your blood pressure, your weight, how well you are sleeping and so forth. Obviously hemo is a special concern… get it tested two or three times minimum on 100mg before moving further.The “good” vs. “safe” thing is misleading in your situation. Your UA was recently much higher so you wouldn’t be safe regardless of your test results.
In light of your test results, 100mg febux is highly likely to be sufficient to cure your gout in the long run if you stick to a decent diet and stay clear of alcohol as well as other diuretics. There’s of course the chance you are a special case but the only studies I remember reading in which a few patients didn’t heal while testing at 350 umol/l or less were looking at bone disease (which is known to develop after successful ULT anyway). So the issue as I see it is: if your lingering symptoms aren’t giving you too much trouble and you aren’t endangering your health by taking anti-inflammatories all the time, endangering it with poorly-tested febuxostat doses seems unwise. On the other hand, if more febuxostat might help you get off other drugs, that would be a different matter…
And if there was something fairly safe your could do to lower your SUA further, it’d be worth trying. So if you haven’t already given a good look at your dairy and minerals consumption… well, here’s a new year resolution for you. Alternatively, see if you can find a doctor who has experience with combination therapies (XOI+excretion booster). -
April 22, 2019 at 1:56 pm #8975Participant
@nobody and @Keith..
My my my… what a period of time has passed since our last encounter.2019 has been a roller-coaster and is finally settling down. tawrikt I’m still waiting for that email stating when your coming over to the small island so I can buy you a coffee (as you know, I stopped drinking long long ago) 🙂
Keith I’ve taken a brief look at a few posts and haven’t seen your presence much. I’m hoping your still good and well and that this forum isn’t just about living from some server in a cupboard in the attic..! Let me know if you need help maintaining the site or if I can help with the tech side.
I wanted to give you both a little update.
So as you both know it’s been tricky times with my situation. We will all know in around 3 months if the blood medication I have been taking since last year is in fact a placebo or is the real thing and it just didn’t work. If it was the placebo, well… that opens a new avenue all over again and we can deal with it then. As we concluded last time I have stuck firmly with the 100mgs Febuxostat ignoring my primary rheumatologist advice to move to 120mgs (more on that later though).As you correctly advised, the UA levels started to drop naturally without changing my dose or dietary habits around January this year. They have spiked twice which is something I’d like to ask you about. So to the results:
Nov 18 – 340
Nov 18 – 378 (tested twice in this month)
Dec 18 – 374
Jan 19 – 353
Feb 19 – 319
Feb 19 – 392 (tested twice in this month)
Mar 19 – 349
Apr 19 – 327The 392 spike in February seemed to have been noise but the 349 result in March may actually mean the February 319 result was a fluke. Taking the results in general however (340+378+374+353+319+392+349+327) / 8 = 314 [strictly average].
So it seems the extra 20mgs that we added at the end of October 2018 reduced UA levels by only around 20 or so which as you rightly said (diminishing return).
In light of the above my rheumatologist has suggested to increase the dose slightly more by alternating days of 120mgs and 80mgs. He doesn’t want to move into 120mgs daily just yet. Argument being to maximise any possible dosing technique in order to get consistent 330ummol and below results whilst leaving 120mgs daily as a final option.
I’m not too sure what to do? I just don’t want my gout to be getting insidiously worse with these erratic results (unless you think they are within safe values to play the waiting game a little longer).
One last thing, has anyone heard of MSM (methylsulphonylmethane) or Organic Sulfar? I’ve been made aware that it helps with pain relief of bones and joints which I still experience quiet often whilst I silently keep telling myself (or wishfully think) the pain is only there because of crystal dissolution and will eventually go away…..
Thanks!
-
April 22, 2019 at 3:56 pm #8976Participant
Hi again!
I’m glad you didn’t disappear because you got a CVE from febuxostat. This is the most controversial thing about this drug.
You almost certainly still have a significant amount of solid UA in your system. This could cause spikes and I don’t think they’re a concern. The therapeutic targets include a safety margin so it’s OK if you exceed them occasionally. Certainly I used to have a lot more variance in my results when the lowest result I could achieve was between 310 and 320 and I still had serious attacks. I guess issues with febuxostat absorption might also explain the spikes (maybe take a look at what you’re eating or drinking around the time you take your dose).
I doubt you really need 120mg but the side effects shouldn’t be much worse than 100mg and increasing your dose might well get you cured faster. You’ve also been on the stuff long enough that slow-onset side effects ought to have shown up by now. I assume there’s no sign of stress in your liver function tests for instance (as with UA, don’t bother with “normal” but compare actual numbers). Maybe get your cardiac-vascular system thoroughly checked out before moving on to a higher dose?
I wouldn’t change my dose from one day to the next if it can be avoided. If your doctor doesn’t want to move to 120mg straight away, could they write you a script for a custom dose such as 110mg? Pharmacists should be able to fill custom prescriptions (they are typically used for young children) but I don’t know if the NHS covers that.I don’t have your email by the way. I’m not going to visit your island anytime soon (especially not given current events) but I could still write if I had it.
-
May 6, 2019 at 1:48 pm #8988Participant
Haha! CVE from Febuxostat – what a terrifying thought. Being reasonably high on 100mgs probably wouldn’t surprise me though.
Yes, my previous rheumatologist said something similar with regards to a significant amount of UA remaining in muscles and tissues all over your body. He explained it like a a bus route which had been out of service for months whilst passengers kept accumulating at the bus stops. “Your going to need quite a few buses running on time constantly to get the passenger backlog clear and only then can you adjust the schedule and size of the bus”. I explained to him if these erratic results could just be clusters of crystals dissolving and he said it’s highly unlikely unless tophi is evident. Although I’m not too sure if that’s true because I haven’t changed anything at all in my diet.
I had my most recent hemo blood test a few days ago and the UA result came back at 345ummol which was very disappointing. Lower then 360 yes but higher then 330. The very first rheumatologist I saw wanted me under 360ummol however the second one insists on being under 330ummol.
All evident side effects seem to have settled down (constipation, aches, etc.) and ALT and ALP levels are OK (ALP levels have definitely increased but are still within the normal range [+-20] ). I’ve also just noticed that my AST levels have never been checked after starting Febuxostat and that my hemo hospital doesn’t even check them by default when doing Liver function (how bizarre!) unless that’s normal? From what I understand ALT and ALP are the key numbers for Febuxostat but I’m a little paranoid and worried now. I will get them checked at another hospital once I get a chance to visit my GP.
I too am not too keen in alternating doses but wouldn’t that overall be better then going all out on 120mgs daily or would regular spikes be a concern to cause an attack? Or maybe just go to straight to 120mgs in the hope that I could be off the higher dose quicker?
What would you suggest providing the numbers mentioned above (Liver, UA)?
p.s. How does one even know when these deposits are all gone to reduce the dose and rule out possible spikes anyway?
Thank you so much mate.
Finally, let’s close the gap on relying on this forum to maintain contact – what would be the best way get my email to you? temp email sites?
Thanks again buddy.
-
May 6, 2019 at 11:17 pm #8990Participant
I don’t think dietary changes have much to do with how much liquid or solid UA there is in your tissues. While uric acid is definitely found in significant amounts in solution outside of the blood, I have found doctors to be unaware of the modern evidence regarding crystals. Not that it matters: whether small crystals would show up with expensive imagery or not is irrelevant to your treatment at this stage.
You never know when all the crystals are gone. You can only guess. And I would recommend not lowering your dose immediately after they’re all gone anyway (see the other long thread I posted in recently). In any case, it’s too early to concern yourself with this. You’re clearly not out of the woods yet.I found the ALT/AST ratio more useful than AST alone though I suppose the absolute value might be important to deal with different issues. Either way, I don’t understand why they don’t test AST. I suppose ALT is the number most likely to become “abnormal” but AST is necessary for a more cogent interpretation of test results (my ALT has typically been “abnormal” even when I didn’t take any drug).
I got one or two high ALP results but that number has been pretty noisy in my case.You could always take a small bit off a 120mg pill every day instead of alternating. It would be imprecise but you’d still get smaller daily variations. It’s not so much the UA variations which worry me but the side-effects. Maybe this is an unwarranted concern but if our bodies are better able to process a steady dose, that would be one fewer potential cause for these rare but nasty side-effects which might possibly be associated with febuxostat (the evidence is quite weak so far).
That said, my guess is that you’d handle 120mg per day just fine. You could always lower your dose later. But that’s only a guess and high febuxostat does aren’t that well-tested…I believe I have previously suggested you simply post your email here if you want me to write. Posts can be edited so your email wouldn’t have to stay up forever. Yes, you could set up a temporary email address and add it to your email client (if you use one) or forward it to your main email account (if your webmail provider offers that feature) but I’m not sure it’s worth the bother. I certainly wouldn’t recommend one of these services which requires you to check your email on their website (that’s only good when you know you’re going to get an email right away).
There are of course other ways to exchange information or chat but I don’t suppose you use IRC or GPG for instance. -
July 1, 2019 at 3:35 pm #9011Participant
Deleted.
-
July 1, 2019 at 4:39 pm #9012Participant
Let me know if my email didn’t get through (but check your spam folder first).
-
July 1, 2019 at 6:30 pm #9013Participant
received and responded! 🙂
-
-
AuthorPosts
The forum ‘Help My Gout! The Gout Forum’ is closed to new topics and replies.