Stopping Gout Together › Forums › Help My Gout! The Gout Forum › The quarterly Febuxostat and Colchicine update!
Tagged: Adenuric/Febuxostat/Uloric Forum Topics, Colchicine Combination Questions, Forum for Gout Patients, Xanthine and Gout Forum
- This topic has 32 replies, 3 voices, and was last updated 4 years, 7 months ago by
nobody.
-
AuthorPosts
-
-
August 2, 2018 at 6:47 pm #7488
d q
Participant
@Keith , @nobody! How are you guys! I haven’t been around the boards much due to work commitments and for some medical research purposes. Its been what, two months or so since I last updated you both? Does time go quicker when your having fun? Well I can safely say I haven’t been having too much of it. Anyway I have some interesting news for you;
So I finally moved up to 80mgs of Febuxostat and the last 4 results on this dose including that paradoxical result is:
18th April – 388 ummol (60mgs)
23rd May – 413 ummol (80mgs) <— Strange result
18th June – 377 ummol (80mgs)
11th July – 360 ummol (80mgs)Now my rheumatologist which I saw a few weeks ago recommended I go to 120mgs as 377 ummol at the time was a little to high for he’s liking. I haven’t decided I want to do this just yet as there are upcoming new medications for my blood condition which could potentially reduce Uric Acid levels naturally as a result. In any case that will require time to test and time to market so that leaves me in this tricky position. I’m not too sure if I should press on up to 120mgs despite the urate having dropped to 360 ummol without a change in dose 3 weeks after the 377 ummol result. I remember we once said as crystals dissolve the level should generally go up first and then slowly come down as there is less and less in the tissues, joints and muscles which may explain the increase and then the steady decrease. Is this correct? If not, any other explanation?
Secondly, unfortunately I had a toenail infection sometime last week and went to see my GP for some advice in which she gave me some antibiotics and told me to soak he foot in salt water twice a day to help clear up the infection quicker. I did that and by the second day in the evening I could feel something wasn’t right with my foot. Pain was no longer only at the toenail site but was spreading slightly. I took no risks and started with the Colchicine, fast forward 2 hours and I knew this is turning into a gout attack. Took a second Colchicine 6 hours later and woke up to pretty much the start of a gout attack. 6 hours later saw me taking the third Colchicine finally hitting the maximum dose of 2mg for the day. I hit hard the second day with the first and second tablet 6 hours apart but by the end of that day I felt the attack was quickly resolving itself and stopped taking the stuff. The third day saw further recovery and by the fourth 90% of the entire attack has abated with only slight inflammation left.
Now I have never had an attack that has lasted only 4 days EVER, 10 days is the least let alone the magnitude of pain difference. On the other hand I have never used colchicine for an attack and only ever used Naproxen. The question that had me puzzled is could this be a result of the Colchicine or is one more inclined to believe this is due to the lower uric acid levels over the last few months causing the attack to be relatively fast and mild? I mean from what I understand 360-370 isn’t exactly low for someone trying to lower their UA levels but could this be playing a part? My other worry was maybe this is a gout hell experience (crystals forming and dissolving) being in that 360-370 zone..? Does the warm salt water over two days have a part in this?
P.s. this is the right foot which hasn’t seen an attack since 2015.
Thanks guys..!
Which Gout Medication Do I Need?
-
August 2, 2018 at 10:56 pm #7489
nobody
ParticipantI never had an attack lasting more than 4 days while taking that much colchicine, whether I was on ULT or not. I thankfully didn’t have cause to test that statement properly so take it with a grain of salt but, my experience aside, stopping attacks within 3 or 4 days is what colchicine is supposed to do when you take enough.
I don’t know if I would have dared to take colchicine if I had an infection but I’m glad to read it didn’t seem to have hampered your immune system’s ability to terminate the infection. Maybe it was effectively resolved by the time you started taking the pills.I never tried putting salt in the foot bath.
Don’t underestimate random variations as an explanations for small changes in SUA test results. 413 isn’t far from 388. And yeah, your average test result should trend down a bit without a dose change.
You could try 100mg if there’s no sign of your system being stressed by 80mg (liver, hemo and so forth) but you’d probably still face a bunch of attacks if you managed to drive your SUA way down. 120mg wouldn’t be a cure-all.Last but not least, I’m overdue for a blood test but I seem to be doing OK. Thanks for asking.
That reminds me I should also check my BP from time to time. And floss too. -
August 3, 2018 at 11:50 am #7499Participant
I never had an attack lasting more than 4 days while taking that much colchicine, whether I was on ULT or not. I thankfully didn’t have cause to test that statement properly so take it with a grain of salt but, my experience aside, stopping attacks within 3 or 4 days is what colchicine is supposed to do when you take enough.
Now had I have known what pain relief Colchicine brings I would have taken the whole bottle of that stuff. My second attack put me out for 2 weeks almost. To be honest though I’m not entirely convinced it was just the Colchicine. I really do believe the lower UA levels are playing a part. After all, my levels have been between 360-380 ummol (except for that 413 result when starting 80mgs).
The antibiotics were a precautionary measure and were started a day after the Colchicine so maybe they actually kicked in as two factor protection [one against the possibility of the toenail infection and one the other as protection from any immune drop Colchicine inflicts.]
I never tried putting salt in the foot bath.
This is indeed a tricky one as Epsom salt brought me pain relief last time maybe table salt does the opposite and potentially helps loosen crystals faster. Who knows.
Don’t underestimate random variations as an explanations for small changes in SUA test results. 413 isn’t far from 388.
Very true sir however 413 to 360 is indeed a fair drop without a dose change.
100mgs is definitely on the cards. I’ve started this new blood medication that could potentially be a game changer but that will take at least 6 weeks to see a change. I’m not too sure what to do! Go up to 100mgs or wait another 5 weeks or so and see if this drug makes a difference! What do you think? Not to sure what you mean by 120mgs won’t be a cure-all btw..? Lastly, face more attacks if I drop my SUA lower down? What’s that supposed to mean! lol.. I thought doing this very gradually would potentially keep that all smooth! i.e. Sticking at 360 for a few months then targetting 340, 320, etc? That was one of my worries. Are crystals actually dissolving at 360 or forming?I too am due my blood test next week so we shall compare and contrast next week sir.. I’m popping down to the shops, floss, anything else mate? 🙂
-
August 3, 2018 at 7:16 pm #7500Participant
I think you should change only one thing at a time. If you just started the blood medication, I’d wait at least until your next blood test to change your febuxostat dose.
I meant that 120mg won’t cure your gout overnight. Getting rid of uric acid deposits will take time regardless.
80mg could do the job. 100mg would probably do a better job. After that, it’s not clear the benefits of a higher dose would outweigh the risks. Keep in mind 80mg is already more than the people who developped the drug are comfortable recommending. Your circumstances required drastic measures but my opinion is that 100mg would be drastic enough. Certainly no evidence to the contrary has as of yet been put forth.Crystals shouldn’t form at 360 or 388 for that matter.
Thing is, your SUA varies and will sometimes be well above that (for instance when largish crystals dissolve). Hopefully it will never be high enough for long enough for crystals to develop. I guess the uric acid in your blood could still occasionally become concentrated enough to react with your immune system but that’s no big deal. If that ends up triggering an attack rather than mild and harmless swelling, it’s only because you still have actual crystals hidden in your joints and bones.I haven’t even scheduled an appointment. There’s no way I’d be able to get a blood test next week, even if I thought it would be of any use and half of the med techs weren’t on vacation.
Sine you ask so nicely, dentists over here recommend you also get yourself some fluor gel (do not let children get ahold of the stuff, blah blah). You should use it with the floss but most of us are too lazy for that so we use it like toothpaste instead. -
August 4, 2018 at 7:22 pm #7501Participant
yep, absolutely right. I’ve slept over it and decided to stick to the 80mg and will see how the new blood medication works out. From a theoretical stand point it should reduce UA but in reality standpoint who knows. I’m due my next dose in a few days and the results should be visible around a month later. If there is no benefit then 100mgs will definitely be the way forward.
Agreed, 120mgs definitely won’t be an overnight cure neither will 900mgs of Alo but at least its a movement in the right direction (providing liver and hemo hold up – which thankfully seems to be the case even at 80mgs). http://drugs.com and http://fda.gov stipulate as you say 40mg with 80mgs being the maximum whereas http://nice.org.uk says 120mg may be considered if 360ummol cannot be achieved. I’m not too sure why the UK has a higher max dose level as normally they are more cautious and slow?
I haven’t done much research on saturation/crystallisation points and had a quick look today. It seems 408ummol / 6.8 mg/dl is the number you want to stay below if you don’t want crystals forming (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3975080/) [but temperature has a huge role]. On the other hand however as you say crystals may be dissolving at 360-380 albeit probably very slowly unfortunately. I’m also aware that 360-380 is so close to the edge that any slight food ‘break’ may cause that spike and a bunch of crystals may form again. The gout attack I have seems to have settled down 95% however I’m getting stone like pressure on the middle of my foot. Not at the gout site but more towards the centre toes. I’m not to sure what all that may be about. Crystals dissolving at the centre toe joints / if they even accumulate there too? Do you occasionally just take a Colchicine tablet when you feel any sort of foot pain as a precautionary measure and for how long or do you just take it when you are almost sure the pain is gout related and take no risks regardless?
On an entirely different note I forgot to mention I finally managed to get a 24hr uric acid test done. Here are the results of that;
Urine Output (24 hours) = 2.5 litres.
Urine Urate Output = 2.4mmol/24hr <— The scale for this is: 1.2-5.9
Urine Urate = 0.95A quick google / conversation on those numbers show that the urate output is actually normal. So that’s finally, after 3 years, pretty much closed that chapter of my worry on being an under-excreter. It’s taken 4 doctors to finally get that test done. I know it doesn’t change treatment options but I guess it gets me closure.
So how has your UA levels / Diab levels coming along? My father had he’s usual bi-yearly DB tests recently. We are waiting to here back. flour-gel ey? I may just look into that sir. LOL about the toothpaste. If you visited even the smallest of chemists here mate you will find that there are more brands, colours, packages, textures and ‘mint’ flavours then the amount of medications that are available in the pharmacy section. It may be the case that you can even find that rare hipster toothpaste yet you may not find Colchicine!
😉-
August 7, 2018 at 11:44 am #7512
 Keith TaylorParticipant
Keith TaylorParticipantYou need to be aware of the context of that PubMed reference (The Crystallization of Monosodium Urate). Because it is focused on lab principles that affect how and when uric acid crystals form or dissolve. But for practical gout treatment, we need to make uric acid safe. So the guidelines that I refer to in my earlier reply (British Society for Rheumatology and British Health Professionals in Rheumatology guideline for the management of gout.) make it clear that 350 μmol/L is safe but 300 is safer. My interpretation of that is that if you struggle to get down to 300 because of other factors then 350 should be OK. But 300 is better. Which is presumably why your rheumatologist suggests increasing the dose.
Obviously, febuxostat always needs to be checked with liver function tests. So make sure you get that irrespective of staying on 80mg or switching to 120mg per day.
I agree with Nobody on the uric acid excretion test. What’s the point if your excretion rates are affected by febuxostat? Maybe the doc has some comparative results for febuxostat patients?
-
August 10, 2018 at 10:18 pm #7598Participant
Hi @Keith
Yes, laboratory based environments are completely different and as you say and that is probably why my rheumatologist wants me under 360 at all costs with a ‘if possible’ aim to get me to a 300.
Thankfully all my regular blood tests conducted for my haematological condition always include FBC, liver and kidney function tests so it is being monitored by both rheumatologist and haematologist.
The 24hr urate excretion test was in addition to other tests the haematologist wanted to conduct for various other reasons. It was never there to alter the treatment method. In any case, from what I understand Febuxostat does not increase uric acid excretion through urine so checking what the capacity of excretion rate does have its benefits. For e.g. if the excretion rate was low, we would at least know that the blood condition might not be the only reason for high urate values. Does Febuxostat act on the kidney’s to excrete more urate too? If so do you have any articles pointing to numbers? That would be very interesting!
Thanks buddy.
-
-
August 5, 2018 at 5:22 am #7502Participant
Like I said, I’m overdue for a blood test so I have no news about my test results. I wouldn’t be overdue if there was a real concern though.
I haven’t used colchicine in quite some time but in your situation, sure: I’d occasionally take colchicine as a precaution. Obviously there are many causes for foot pain so don’t take it for ANY foot pain. And I wouldn’t necessarily have waited for actual pain to develop. You should be able to guess what odd foot feelings might possibly be related to incoming gout by now.
Like I said, the one thing I used to be paranoid about when I took colchicine was infections. I wouldn’t have taken it as a precaution if I had any kind of bleeding for instance. So colchicine made for a great excuse to avoid flossing.
I’m not sure what you’re asking about the center toes but you can of course get gout on any toe joint, not just the largest where gout is typically very painful. And between the thickest parts of the toe joints, you’ve got stuff which may or may not be technically joint tissue but it’s also gout-prone anyway.I’m surprised you got an excretion test now. I was told you’re supposed to go off UA meds for a while before you can get a useful result.
In any case I don’t think it matters whether your result is “normal”. People with “normal” uric acid are still given allo to cure their gout and I except people with excretion on the weak side of “normal” relative to their SUA would also benefit from excretion boosters.As to the febuxostat dosage mess, profiteering is evidently to blame for it.
The UK has less resources than the US to deal with uncommon drugs. It’s not enough to have a public health system. The people in charge also need to be willing and able to question self-serving information offered by foreigners. -
August 5, 2018 at 1:26 pm #7503Participant
Yes, maybe I should have tested and even used Colchicine earlier on. Heck, some may say I should have even taken a tablet a day when starting Febuxostat and gone straight to 80mgs working my way backwards if there were issues or changes. In all honesty however nothing major has happened going slowly upwards apart from that mild attack a few days ago. I started Febuxostat in November 2017 and have been titrating slowly and cautiously and I have no regrets.
I’m not too sure a 24hr UA test needs to be done when your off UA therapy. It’s a simple case of your kidneys removing adequate levels from your blood and if you have less of it in your system as a result of ULT then you will generally have less excreted, if more was in the blood you would still fall under the normal rate. Besides, I’ve had this discussion with my rheumatologists both of which have told me that those drugs are generally avoided wherever possible.
I know your very cryptic and occasionally worry too much about giving out any information about your particular situation especially when it comes to certain questions but how long have you actually been on Febuxostat and when was your last gout attack? [surely you cannot think I can take you to court for such an answer] 😉
My blood test is next week and am a little anxious! I am really hoping to see a number less then 360, even remaining at 360 will bring comfort!
Otherwise it seems your condition is generally stable – I’m delighted for you mate. I hope that continues to be the case going forward. Either way, if your ever over in the UK and don’t want to remain nobody then please feel free to message for a real catch up. It would be interesting meet for sure 🙂
-
August 5, 2018 at 2:32 pm #7504Participant
Let me be “very cryptic” then: I got some fairly nasty attacks about 3 months after getting my SUA consistently under 300 with febuxostat. Since then, I’ve only experienced minor symptoms.
I’m not sure what symptoms deserve the name “attack”. Certainly it’s been quite some time since I have experienced textbook gout attacks (swelling, redness and pain at rest). On occasion the minor gout-like symptoms can be most annoying (too much swelling to put on my shoes for instance) but that’s nothing in comparison to what I had gotten used to.
The frequency of these annoyances has slowly been decreasing but it’s too early to make definitive claims about the efficacy of ULT in my case. Hopefully by 2020 I’ll feel confident enough to give a useful account of my particular situation and to travel without a set of emergency drugs. In the meantime, best get your timetable from people who have been successful in curing their arthritis.Though I’d much prefer visiting England (or some other British republic), assuming this forum still works by then I’d have no problem throwing you an @ should I cross the Channel for the first time in decades.
-
August 7, 2018 at 11:50 am #7513Keith TaylorParticipant
or some other British republic
Yorkshire?
assuming this forum still works by then
As I get older I think more and more about a legacy solution for this forum when I can no longer support it. So the time for that to start is probably now.
If anyone has any ideas for how that might happen, please start a new topic.
-
August 7, 2018 at 4:55 pm #7521Participant
If I’m not mistaken, Yorkshire has yet to get international recognition for its football team. Do they even shoot crime procedurals in whatever language people used to speak over there?
-
August 7, 2018 at 10:24 pm #7525Participant
@nobody Yes, when I got under 300 with allopurinol before stopping it I got the worst attack ever and even today I have lingering pain with good days and bad days. MRI’s and X-Rays show no damage however I’m almost certain something is wrong. I need to ask my rheumatologist but do you know if the possibility of short month course of low dose Naproxen or colchicine can possibly have an impact? He wants me under the UK therapeutical limit of <360 whilst keeping the option open of even possibly getting me to the European therapeutical limit of <300 (if I understood him correctly). Is <300 the magic number in your country?
Those minor gout symptoms you get which luckily for you are decreasing are pretty much what I get and keeps me constantly worried and in some cases keeps me from enjoying certain aspects of life. I don’t get swelling but I just get pains around the joint all the time which keeps me thinking should I go out, travel, etc. or just stay home and keep it elevated. Anxious an attack is coming up.
Well good luck with 2020 mate. Its ultimately its physiology isn’t it? Reduce UA, wait a few years ffs and done? (well that’s what i’m banking on). Out of curiosity how do you deal with these annoyances by the way? Colchicine? Naproxen? etc?
Well we’re going to have to have a coffee either before this shop closes. Find me a way to safely get my contact details across and I would happily come over to visit you.. Don’t give me a complicated to that specific question now nobody 🙂
p.s. excuse any grammar or linguistic mistakes, I typed this really fast on a portable device.
-
August 8, 2018 at 7:19 am #7527Participant
re: ffs
Please don’t assume that you’ll need to wait a few years for your symptoms to go away. You didn’t spend anywhere as much time as I did with untreated symptoms. And I was also taking into account the time necessary to become confident that symptoms are gone for good.
I haven’t kept a foot elevated or used pills for symptoms in quite a while (I only keep them around, just in case). It’s really not that bad. Keeping myself “from enjoying certain aspects of life” has long become a habit anyway.As to your “specific question” which isn’t actually a question (hence the smiley?), it comes down to this: could anybody fool you into thinking they were nobody? If not, simply post an email address of your own instead of asking me for the moon. Artful obfuscation will prevent software from harvesting it for spam. There’s no guarantee I’ll see your email as opposed to anybody else’s but I don’t mind sending emails unsafely. Over time, we may come to trust that we indeed have each other’s email.
There’s no technical trick that would allow two nobodies who don’t know each other at all to establish any kind of secure channel over a public forum. Thankfully, we don’t need a secure channel. All we need is patience. -
August 11, 2018 at 11:10 am #7601Participant
@nobody haha – you are indeed an interesting character! no worries mate, I’ll kick of the process in a separate thread and forum and we’ll take it from there. Relax a little my friend.. Put a little faith in your friend [hopefully anyway] across the pond. A dedication of a little patience will indeed be the proof 🙂
p.s. Curiosity killed the cat;
1. how long roughly did you keep it untreated?
2. exactly why I want this s*** behind me. There is so much I still want to do. It was only a 5 years ago I didn’t know what gout even was and enjoyed work, life (in most cases anyway), etc.
-
-
August 7, 2018 at 11:11 am #7511Keith TaylorParticipant
Hi James, thanks for the update.
I’m also of the opinion that your strange 413 μmol/L uric acid test result is within the bounds of usual variations (How Your Uric Acid Level Changes). Because there are lots of other factors at play here, besides the action of febuxostat (Uloric). For example, time of day, time since last meal, amount of exertion. But also the fact that uric acid crystal debulking is not a linear process. So a cache of crystals that have been well hidden by immune reactions and subsequent mineralization/calcification/etc can spontaneously dissolve and temporarily raise uric acid levels. As Nobody notes, this often happens months after getting uric acid safe.
I’d go as far as saying that linear trends in uric acid test results are highly unlikely. So I tend to ignore the highest and lowest. Then look for average trends.
On colchicine, I’m also in agreement that 4 days seems about what you would expect to stop gout pain. But colchicine does not act on existing inflammation, as it restricts inflammation spreading. So I would support it with naproxen to get faster relief.
-
August 10, 2018 at 9:35 pm #7597Participant
Hello @Keith – good to finally hear from you mate. I see you don’t really spend much time on the boards any more. Any particular reason?
Yes, that 413ummol was definitely a strange result and happened right after the increase so I assume the UA levels dropped rapidly and something immediately dissolved and returned that result. In any case there does seem to be a gradual overall decrease. Well maybe just until another cache of crystals dissolve that is. Unfortunately I couldn’t do my blood test this week and I will now be doing it next week. I guess that result should give us a good indication as to where we may be heading especially since I would have been taking this new blood medication for over 5 weeks. To be honest I’m really hoping that I don’t need to increase my Febuxostat dose further.
From what I understand 80mgs of Febuxostat is ‘loosely and usually’ compared to 300mgs of Allopurinol. I remember I required 400mgs of Allopurinol to get to 283ummol back when I tried it last year. Maybe 120mgs of Febuxostat is the equivalent to roughly 400mgs dose of Allopurinol?
When you say support with Naproxen, do you mean take Colchicine followed by my usual dose of 500mgs twice a day? Or should the dose be decreased when taking it with Colchicine?
The new trial of the medication is supposed to correct late stage erythropoiesis (maturation of red blood cells). This technically means less defective or non-functional red cells floating around which effectively results in less uric acid from their premature death. Let me know if you wish to explain this in greater detail however.
Cheers mate.
@nobody if you have comments on the Allopurinol vs Febuxostat numbers please comment pal. Thanks! -
August 11, 2018 at 5:44 am #7599Participant
Way off the mark. 40mg febuxostat is supposedly like 400mg allopurinol… or possibly more like 350mg.
Allopurinol may have done something else to your body than simply inhibiting xanthine oxidase. Or it was a coincidence and your hemo just happened to drop around that time. Either way, your 283 result was probably in no small part due to your hemo situation. -
August 11, 2018 at 10:55 am #7600Participant
Wow, that is indeed way off the mark! Yes, my haematologist still believes till this day that hemo drop was due to some sort of inflammation or infection. They are simply not convinced it was the Alo. One of hypothesis was since uric acid acts as a powerful anti-oxidant and such low levels may have impacted the already fragile red cells and in my case causing accelerated cell death OR it was causing bone marrow suppression causing uric acid to drop heavily simply because there are less red cells in the blood to start with. It was a little ironic with each dose increase (and uric acid decrease) did we see a hemo drop. The first major hemo drop happened at 336ummol and we aren’t there yet with Febuxostat. Either way it may be an option to explore if Febuxostat cant control the situation. I guess the way to look at it is if they make a 120mg pill then some people just need that much.. Worst goes to worst I’ll live a little shorter but a lot healthier (go figure) 🙂
-
August 11, 2018 at 11:43 am #7602Participant
That 120mg pill also happens to put more money in some people’s pockets. And it nevertheless seems to have been withdrawn from some markets…
I’m sure some people do well on 120mg but you better be careful. Loads more people have taken up to 80mg daily than 120mg, and for longer to boot since they didn’t make pills stronger than 40mg at first.As to your other q., a quick reminder (we already went over this): I first had typical gout symptoms more than 10 years before I was able to take a XOI for long enough that we might call it treatment. I was able to get halfway decent numbers for a while by watching what I ate and drank though.
-
August 11, 2018 at 6:48 pm #7603Participant
Well, let’s be honest, I’m shot and bleeding either way really. Take the pill and burn my heart and liver a decade or two earlier but have mobility OR have serious gouty Arthritis by mid 40’s wishing I did take it;
1. Food alone won’t solve it, or even get close.
2. Combination therapy with excretion drugs have more worrying side effects and have to be taken twice a day.
3. Allopurinol wont work for me (Maybe try this again one day)The only really viable options are;
1. Wait to see if 80mgs keeps bringing the level down naturally as it has been.
2. Take 90mg-100mg rather then 120mg
3. See if this new blood medication trial has an impact (my best shot really)
4. Sticking with 80mg @ 360-380 and go through a slow slow dissolve?Some die taking these drugs, some die because they decided not to take them 🙂
Consider yourself very lucky @nobody. Your slice of the gout cake is indeed tiny -
August 12, 2018 at 8:32 am #7605Keith TaylorParticipant
Febuxostat vs Allopurinol Mortality
Some die taking these drugs, some die because they decided not to take them
I have an alternate view. Unfortunately, I can’t find the exact studies to back up my theory. But I believe that long-term gout patients generally have a health advantage. Because they are more likely to get regular health checks. So early signs of other health problems should be spotted and corrected earlier. Of course, that assumes the patient has the sense to insist that appropriate tests are done alongside uric acid monitoring.
In my previous message, I mentioned a study that investigates mortality rates. And other studies show different comparisons. But differences are small. And statistics only show averages – not the personal situation where you take better than average care for your own health.
Finally, since we’re looking at comparatives, I think your uric acid levels are good compared to many gout patients. Most studies show that less than 30% get below 360 μmol/L. Primarily because most doctors can’t get past the mental block of increasing dose once patients get average uric acid scores around 400-420. Is it time to worry less and get back to “5 years ago I didn’t know what gout even was and enjoyed work, life (in most cases anyway)”
-
August 12, 2018 at 8:08 am #7604Keith TaylorParticipant
Febuxostat vs Allopurinol Comparative Doses
Coburn, Brian W., Kaleb Michaud, Debra A. Bergman, and Ted R. Mikuls. “Allopurinol Dose Escalation and Mortality among Patients with Gout: A National Propensity‐Matched Cohort Study.” Arthritis & Rheumatology (2018).
we estimated that the three febuxostat doses observed during follow-up (40, 80, and 120 mg/day) were approximately equivalent to 300, 600, and 900 mg/day of allopurinol, respectively
That estimate is based on their analysis of the clinical trials results in:
Becker, Michael A., H. Ralph Schumacher, Luis R. Espinoza, Alvin F. Wells, Patricia MacDonald, Eric Lloyd, and Christopher Lademacher. “The urate-lowering efficacy and safety of febuxostat in the treatment of the hyperuricemia of gout: the CONFIRMS trial.” Arthritis research & therapy 12, no. 2 (2010): R63.But, since these two drugs affect different pathways, I would expect results to vary between individuals.
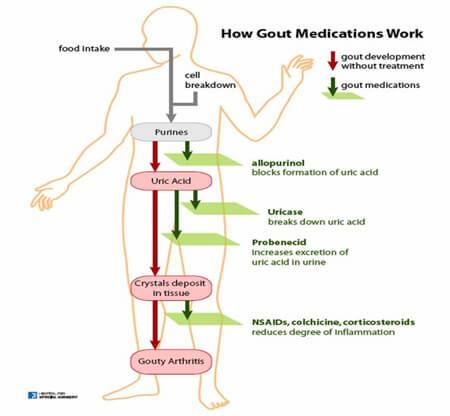
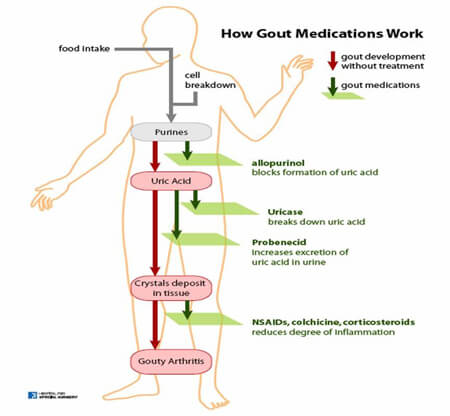
Apart from that, the latest trends seem to be combining xanthine oxidase inhibitors with uricosurics. Which is explained rather beautifully in the final step of http://changegout.com/explore-gout
There’s also an interesting film on that website.
-
-
August 7, 2018 at 11:52 am #7514Keith TaylorParticipant
And finally (for now)
there are upcoming new medications for my blood condition which could potentially reduce Uric Acid levels naturally as a result
What medication is that @d_q ?
-
August 19, 2018 at 8:49 pm #7661Participant
@Keith – Your comments make very valid points
I have an alternate view. Unfortunately, I can’t find the exact studies to back up my theory. But I believe that long-term gout patients generally have a health advantage. Because they are more likely to get regular health checks.
You know, I never once thought of it like that. I’m generally watched over by my haematologist but it does make perfect sense.
Primarily because most doctors can’t get past the mental block of increasing dose once patients get average uric acid scores around 400-420
This is absolutely without a doubt spot on as my second opinion rheumatologist was “happy to see that my uric acid levels are now within the normal range at 413ummol” -What a load of garbage.
Is it time to worry less and get back to “5 years ago I didn’t know what gout even was and enjoyed work, life (in most cases anyway)”
Believe me buddy I wish it was a simple as that. Every time I get a feeling of pain I panic and limit activities for that day. I would love to be able to just go on holiday and not worry about all of this. I just wish it would end.
p.s. @Keith, what is your current gout situation? Are you still on your Allopurinol break? How do you manage it these days?
-
August 19, 2018 at 9:35 pm #7663Participant
Just an update on this update – I took the blood test a few days ago and the UA levels have dropped further to 343 ummol without me making a single dose change.
18th April – 388 ummol (60mgs)
23rd May – 413 ummol (80mgs) <— Strange result
18th June – 377 ummol (80mgs)
11th July – 360 ummol (80mgs)
15th August – 343 ummol (80mgs)Liver markers and Kidney markers are fine so far. I doubt its the new blood medication working because the targetted haematological values haven’t changed yet as they generally require a little more time under normal circumstances (unless for some reason the UA levels are getting impacted first).
So that leaves me in a really tricky situation!
Why are UA levels continuing to fall since May even without increasing my dose?
Is this an example of less crystals to dissolve or just a lucky one off?
I was preparing to start 100mgs and now I’m really not so sure what to do.
Maybe get tested again? :/I really don’t want to end up in the crystallise/dissolve gout hell situation?
Thanks guys.
-
August 19, 2018 at 9:56 pm #7664Participant
It’s more than just one lucky result, innit?
If you weren’t on a new medication, I would recommend trying 100mg/day.
But since you’re already trying something new, I wouldn’t also change a febuxostat dose which has been stable for some months now. Even if you had no cause to be concerned about side effects, you’re not going to see the effect of this blood medication on your SUA if you also increase your febuxostat dose.There’s little cause to be afraid of “gout hell” at this stage. You’ve already reached the recommended value. It’s not ideal yet and you are of course still at risk of gout but dropping your UA test results under 300 would not magically protect you against gout. You might clean the remaining UA crystals from your system a bit faster with lower SUA among other benefits but I have yet to see any evidence it would make a big difference in your situation. It’s mostly recommended for people who used to have worse gout than us.
What you need most at this stage in my opinion is patience and a powerful set of emergency pills just in case.
-
-
August 23, 2018 at 10:14 am #7687Participant
@nobody – Hello mate. Yep, it is more then just the one 🙂 I’ve decided to keep everything just the way they are for now. If the new medication starts to work on hemo it would show results from around the third dose which is what I’ll be on in a few weeks. I’ll definitely be having another blood test in between however, so I’ll have an update with UA levels then.
Dropping levels to under 300 wouldn’t magically just protect you? That’s bizarre? I would have thought at sub 300 crystals can’t physically be created in the first instance? Educate me on this on buddy?
It’s mostly recommended for people who used to have worse gout than us. Ahh, that’s very interesting! I think I get you. I’m assuming you mean a high UA for a longer period?
patience and a powerful set of emergency pills just in case.
Patience – Gout amongst a very few other life experiences has overtaken all other patience teaching exercises in life. So I guess a few more months or years can’t destroy me further. I wish there was an accurate way of predicting the time left.Powerful set of emergency pills – Oh no.. why is that? I’m assuming because of the lower UA levels attacks will become imminent or is it because of the low buffer between “Good and Gout Hell”. Advise me on this one pal..?
Finally, just out of curiosity, when would one generally be concerned about “gout hell” at the 388 result?
You are the man nobody! 🙂
-
August 23, 2018 at 3:29 pm #7688Participant
I’d say the main point of having reliable emergency drugs with you at all times is as you put it, to worry less and enjoy life.
One advantage you have over me is that it looks like you can handle serious NSAID dosage. Yet it seems you aren’t taking full advantage of that bit of good luck.It doesn’t matter when crystals still manage to form (they shouldn’t be forming at 400 either though it’s more complicated in practice).
Dropping SUA under 300 hasn’t been shown to dissolve old UA crystals anywhere as quickly as we’d like. That’s the problem. The same goes for 250 and so forth. The lower, the better but it’s not clear it makes a big difference beyond a certain point.
And as far as I can tell, it looks like that point depends on how bad your gout is (and in particular on where your UA crytals are, which in turn depends on the SUA you used to have among other things). Mainstream European guidelines also suggest such a relationship (or rather that I’m not alone in entertaining such a notion).I don’t quite subscribe to this “gout hell” notion in the first place but for what it’s worth I think it would mostly be a concern when your tests aren’t consistently under 400.
The effectiveness of your “buffer” is also going to depend on your body’s excretion abilities (urine isn’t the only pathway). So possibly my 350 is your 320? Shit’s complicated.
Only the evolution of your symptoms over the years can tell for sure if your SUA target was the right one. -
August 23, 2018 at 10:18 pm #7689Participant
to worry less and enjoy life.
You know mate, I should apply that more. I’ve been really set back this year. I’ve had ongoing pain, a few disappointing results, and maybe even deflated at times.One advantage you have over me is that it looks like you can handle serious NSAID dosage. Yet it seems you aren’t taking full advantage of that bit of good luck.
In all honesty pal, your probably right with regards to the “not taking full advantage of NSAID” I’m assuming you mean for the lingering pain I currently endure? I only ever took Colchicine once in my gout attack history and it reduced the last attack miraculously to only 4 days. I’m guessing applying maximum dose Naproxen would probably bring that down to 2 days or something?
p.s. Believe me you have many many more advantages.Dropping SUA under 300 hasn’t been shown to dissolve old UA crystals anywhere as quickly as we’d like. That’s the problem. The same goes for 250 and so forth.
Well that’s a relief, at least we’re not trailing along hoping and hoping to get lower UA levels for those “many benefits”. In your opinion and out of curiosity would opting for 340ummol be better then opting for 100mgs of Febux to gain maybe +/-30 ummol less (p.s. I’m just assuming that UA level saving)?
I don’t quite subscribe to this “gout hell” notion in the first place but for what it’s worth I think it would mostly be a concern when your tests aren’t consistently under 400.
Interesting comment. I mean I can see the logic behind gout hell though. It does make sense don’t you think? On the dangerous edge of crystallise and dissolve sort of level.
The effectiveness of your “buffer” is also going to depend on your body’s excretion abilities (urine isn’t the only pathway). So possibly my 350 is your 320? Shit’s complicated.
I love that comment.. I have to admit hitting the good ol’ loo does bring relief on every level..! I believe we excrete 1/3 of our UA through crapping! 🙂
As if I haven’t I asked you enough already in this post so I thought I’d make the last bit informational only.. That abdominal pain I was having? It seems to have become a fart in the wind. Thanks to you in one way or another 🙂
-
August 24, 2018 at 1:06 am #7690Participant
I realize I have advantages. I’m not the one who used to argue that our situations were similar. 🙂
About enjoying life, there have been times when I wanted to die because of my joint troubles. For what it’s worth, after only a few years in “gout hell” my troubles weren’t so bad as to drive me to despair anymore. Maybe I’m a special case, maybe I was suffering from some other disease, whatever. But it looks to me as if lowering one’s SUA into “gout hell” does bring about an improvement, as it should (crystallization is in theory a slow process anyway). Obviously you want more than a mere improvement and you don’t want to wait years so it’s best to lower one’s SUA further down than the edge (as you did).
Now I only need to find some other metabolic tweak to deal with insomnia.As to the following request: “In your opinion and out of curiosity would opting for 340ummol be better then opting for 100mgs of Febux to gain maybe +/-30 ummol less (p.s. I’m just assuming that UA level saving)?”
Not sure what “saving” means here but if your blood med doesn’t end up lowering your UA and you aren’t experiencing a clear improvement in your symptoms after a few months of sub-350 SUA… then I’d try 100mg/day febux.
Every case is different. I can’t know what risks you’d be facing if you increased your febux dose and I can’t know what benefits you’d get by going from 340 to 310 either. What I do know is that time will tell if 340 isn’t low enough.
-
-
August 27, 2018 at 4:42 pm #7693Participant
I realize I have advantages. I’m not the one who used to argue that our situations were similar. 🙂
Yes sir, but we did share a few similar symptoms! That you cannot deny! 🙂About enjoying life, there have been times when I wanted to die because of my joint troubles.
@nobody – believe me mate I know exactly what you mean. It was a feeling of torture and wanting to give in, it was horrible pal. I have to admit, since my last gout attack a few weeks ago, both my feet have been feeling much better. I think its very much a question of keeping your UA under 350 for a period of time. That’s were all that toxic junk starts to clear out of muscles too. I have every bit of belief now that keeping it at this level is as you say beginning to show its advantages.Not sure what “saving”
I knew that wasn’t the right word to use! my bad. Let’s say the blood meds don’t really have a positive impact on UA (next blood test in 10 days), would being at 343ummol generally be better then taking more Febux to get down to let’s say 310 or 315ummol? In any case I believe you’ve answered that by saying it depends on your symptoms which makes sense. I’m assuming symptoms meaning ongoing pain and gout attacks? Reason I am asking is aren’t attacks likely in the first few years – so how does one generally decide if sub 350 is working in a few months? – This would really help knowing.Now I only need to find some other metabolic tweak to deal with insomnia.
My dad suffers the exact same issue, can’t sleep before 4am. I also get the occasional few days depending on stress and family. I try and read (a book) as that really helps sometimes. Have you tried the cocoa and milk approach? 🙂 -
August 27, 2018 at 8:13 pm #7694Participant
Here’s my guesswork: even if you still get attacks, you should notice a trend: on average shorter, less severe and/or less frequent. And you shouldn’t need to wait years to see such a trend clearly (more like 6 months at the outside). To the extent that you also experience less acute symptoms, you should also notice a trend as far as these are concerned. You might have needed to wait years for improvements to become clear if you had only succeeded in lowering your SUA to 400 or so.
That said, just because you’re feeling better doesn’t mean you can’t get a nasty attack out of the blue, especially during the first few months after you start feeling well. There are outliers to any trend. But emergency drugs should resolve such attacks quickly provided you don’t skimp on the doses.I can usually sleep long before 4 AM without difficulty. I just need to stop reading, else I could stay awake through the night. I do sometimes resort to putting something soothing in my stomach though I try not to make a habit of eating sweetened products (or cocoa products, for a different reason).
-
-
AuthorPosts
The forum ‘Help My Gout! The Gout Forum’ is closed to new topics and replies.