Forum Replies Created
-
AuthorPosts
-
 Keith TaylorParticipant
Keith TaylorParticipant
Thank you Mazzaroth man, weird indeed, and very interesting!
I’ve added the images from that study to your post. Also, I had a look for some related studies, and I found 2 similar studies about gout and smoking.
– From Oman in 2008 Serum Uric Acid in Smokers. The authors point out that risk of heart disease rises as uric acid falls. So, probably not a good idea!
– From Britain, in 2014 Cigarette smoking is associated with a reduction in the risk of incident gout: results from the Framingham Heart Study original cohort. I’m uncertain what the authors are suggesting when they say “We do not intend to suggest people take up smoking in order to prevent gout.”Interestingly, in 2006, EULAR, the European rheumatologists, recommended: “3. Associated comorbidity and risk factors such as hyperlipidaemia, hypertension, hyperglycaemia, obesity and smoking should be addressed as an important part of the management of gout.”
Although there is no direct evidence to support smoking as a risk factor for gout, smoking strongly associates with alcohol consumption, which may in turn associate with gout. Importantly, however, smoking is a modifiable risk factor for cardiac and peripheral vascular disease, as well as many other diseases, and therefore needs to be addressed in a holistic approach to patient management.
So, expect smoking to become compulsory for European gout sufferers any day soon. (Let’s keep Brexit in General Discussion ).
I don’t need to include images because I’ve linked to full reports. But, here’s one anyway:
Smoking and Gout? 😉
Keith TaylorParticipantSleep apnea is not easy to diagnose. But there are some hints from this thread about sleeping on your back, feeling tired through the day, and feedback from people who notice you stopping breathing. Anyway, I suggest you use the forum that Stephen suggested. Or, the forum on the websites I mentioned above at http://goutpal.net/forums/topic/found-this-interesting-read/#post-2662
You are right that sleep apnea can be a sole cause of gout for some people. But, for other gout sufferers, it is just a contributing factor.
Keith TaylorParticipantCan I suggest a note of caution re colchicine? Because, I understand there are different attitudes to dosing. But, it’s my belief that doses heavier than 2mg per day are rarely beneficial. So, I suggest looking at the indomethacin dose as well.
You should understand that colchicine is very effective at blocking inflammation from starting, or spreading. But, it does nothing for existing inflammation. Which is why you need strong anti-inflammatories to support colchicine if inflammation has taken hold. Also, in severe cases, you might need a supporting pain-blocker like Tylenol. Or, whatever your doctor or pharmacist recommends.
Keith TaylorParticipantI hope you’ve seen my earlier reply about increasing from 100mg allopurinol in slower stages. You’d normally do that with a pill-splitter. Eg, 100, 150, 200. Start changing weekly, but adjust according to symptoms. So, I recommend you create a Symptoms topic. Then, you can record your gout symptoms and side effects each day.
However, I’m confused about your prescriptions. So, I suggest you start a new diary topic that maintains a list of all your prescription medication. Plus any OTC meds or supplements. Because, your middle paragraph seems to suggest you are taking naproxen and Celebrex at the same time. Which is considered dangerous. Also, why did your doc take you off colchicine?
Keith TaylorParticipantIf I were in this situation, Stephen, I’d take the allopurinol down to 100mg per day. Then, if I tolerated that, I’d increase it in very small amounts – a process known as allopurinol desensitization. Your rheumatologist should be able to decide on the dose increase, and interval.
One reason why I suggest this over febuxostat is because that drug is also associated with dizziness in pre-market trials. Also, allopurinol has a longer safety record, and it is much cheaper.
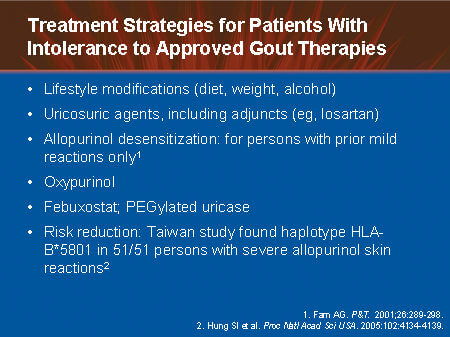
Allopurinol Desensitization is one option for allopurinol intolerance
Keith TaylorParticipantI’m confused why you are asking me what I think about that page. Where is it’s merit? Why is it influential to you?
Insulin spike from oatmeal!?! Really?
Anyway, I guess I should be sensible. Insulin resistance, as far as I know, is not directly related to gout. But, there are strong associations between risks of gout and risks of diabetes. So, let’s look at ” Clinical Benefit of a Short Term Dietary Oatmeal Intervention in Patients with Type 2 Diabetes and Severe Insulin Resistance”. Which is a pilot study from December 20, 2007 Exp Clin Endocrinol Diabetes.
diabetes adapted diet followed by oatmeal intervention achieved a ~40 % reduction of insulin dosage required to achieve controlled glucose levels.
Perhaps more significantly, have you tried searching oatmeal and gout in any recognized scientific resource? I’m biased enough to suggest the best search results come from the search box at the top of all my pages. Also, on that search results page, you get an option to search Google Scholar. Finally, there are other reliable gout science resources, such as PubMed. What do you find if you search ‘oatmeal and gout’? Nothing! Because there is no connection. And, I’m extremely worried about the thought processes that make anyone think there could be a connection.
If you want to get anywhere with gout diet, you have to stop putting individual foods first. Start with a good healthy diet based on whole foods. Especially plants. Once you’ve established that, and got your calorie intake under control, you might look at single foods within the context of your overall diet. In which case, you would compare your suspect food item with one or two alternatives.
I hope you realize that fine-tuning a diet takes a long time. But, each day you work on getting better diet, your uric acid burden increases. That is very dangerous. So, it’s much safer to consider allopurinol, or other uric acid lowering treatment. Because, that buys you time to get your diet sorted, without the risks of permanent joint disease or organ failure. Then, if you improve your diet, and get obesity under control, you might be able to reduce, or even stop, the allopurinol.
Either way, don’t be afraid of porridge.
Keith TaylorParticipantFurther to my last post. Indeed, there has been some more recent research. It tends to confirm that allopurinol is generally helpful to kidneys. But, data is still inconclusive. Anyway, I’ve updated my article to reflect this recent research.
I’ve also take a look at the wider picture of tinnitus. There are many things that can cause it, and often the condition is temporary. So, as always, if tinnitus becomes unbearable, you have to seek medical attention.
We know that gout can affect the ears. Therefore, it seems logical that sudden dissolving of uric acid crystals could cause temporary tinnitus. But, I cannot find any research that supports my theory.
Keith TaylorParticipant“As allopurinol does in fact have some effect on the kidney”
Cindy, everything I’ve read so far suggests that allopurinol helps protect kidneys (and heart). Please can you post the source of your information so that I can check it.
Thanks
PS I based that mainly on what I wrote in Allopurinol Tablets & Kidney Disease. So, I’ll check to see if there is any more recent relevant information. Because that is over 10 years old.
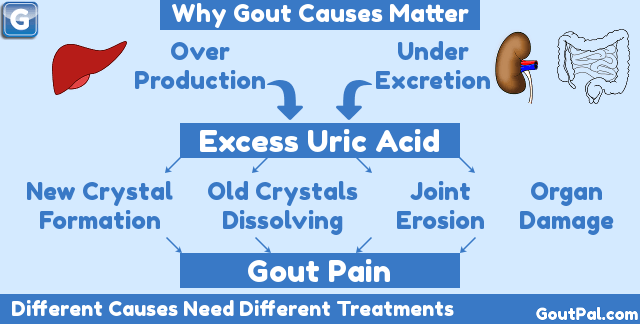
Keith TaylorParticipantThere’s really only one thing that causes gout, and that’s excess uric acid.
Now, it usually takes many years for the excess uric acid to form enough crystals to start gout. So, it’s useful to have some uric acid test result history. Therefore, can you check with your doctor. Then post as much uric acid blood test history as you can get, with dates.
Unfortunately, it’s very difficult to pin down a specific thing that finally pushes your gout to flare up. Also, it’s not very helpful. Because the only way to control gout, is to control uric acid. More importantly, if you do nothing, this is going to get worse. Because, you will find that interval between gout flares gets shorter. Also, more and more joints become affected.
Finally, the good news is, gout is very easy to manage, if you do it right. Also, you are young enough to stop gout before it permanently damages your joints. So, to avoid that, and other potential dangers including kidney disease and heart disease, let’s get your gout under control now.
If you need any help about what to ask your doctor, or how to understand his advice, please ask.
Keith TaylorParticipantYes, you must never stop taking allopurinol once you start it. That is the golden rule of allopurinol that should never be broken.
Except, when you first start, which should be 100mg allopurinol, if you feel you are having a bad reaction to it, contact your doctor immediately. On the label, you should see the warning symptoms that prompt you to stop. Other symptoms might tell you to continue, but tell your doctor.
I won’t bore you with other instances when you might break this golden rule. Because all rules are made to be broken. But, you have to have a complete understanding of the rules, and consequences, before thinking about breaking them.
I’ll start a separate topic about helping you with your gout diary.
Keith TaylorParticipantThat sounds like a good plan, Cindy.
On the issue of tinnitus, you’ve prompted me to review my information. But, I can’t find any more references to allopurinol and tinnitus. So, I added your case to the list at the end of Gout Drugs & tinnitus. As you can see, I don’t know if this is a side-effect, or just a coincidence.
Keith TaylorParticipantPrompted by a recent message about allopurinol and tinnitus, this topic seems the best place for me to summarize my research into the problem. Especially since this is about naproxen and tinnitus. Because, naproxen is a Non Steroidal Anti-Inflammatory Drug. And, NSAIDs are the most common gout drugs associated with tinnitus.
Gout Drugs and Tinnitus Science
There’s a useful 2011 report, “Pharmacological drugs inducing ototoxicity,
vestibular symptoms and tinnitus” that lists the following NSAIDs associated with tinnitus: Aceclofenac; Celecoxib; Dexibuprofene; Dexketoprofene; Diclofenac potassium; Diclofenac sodium; Diclofenac + misoprostol; Etoricoxib; Flurbiprofen; Ibuprofen; Indomethacin; Ketoprofen; Mefenamic acid; Meloxicam; Nabumetone; Naproxen; Piroxicam; Sulindac; Tenoxicam; Tiaprofenic acid. It does not associate allopurinol with gout. But, it does associate it with vertigo.I have only extracted gout drugs from the lists in that report. But, it does include drugs for other conditions that gout sufferers commonly take medications for.
The indomethacin connection is mentioned in the product label as an adverse reaction with incidence greater than 1%. Also, not in the report, is Uloric (febuxostat), where tinnitus is listed on the label as an adverse event with incidence less than 1%.
Tinnitus in the Gout forum
Oct 2009 Diuretics and gout: “Lasix worsens tinnitus”. Lasix is taken for high blood pressure.Sep 2011 I have the allopurinol blues: After switching from allopurinol to Uloric (febuxostat),”I have a history of tinnitus (ringing in the ears) that normally comes and goes every few days, and usually occurs in the evening. Since my first dose of Uloric, the tinnitus has been persistent, and the volume is up a notch”.
May 2012 The Febuxostat Debate: “when i was taking indomethican for gout I was having that problem and I found out that its called tinnitus”.
Aug 2012 The Febuxostat Debate: “Im suffering from one of the listed adverse effects of Fexuxostat but I am most reluctant to stop the medication as it has changed my life for the better. Unfortunately the tinnitus is becoming very difficult to tolerate”. Febuxostat tis the generic name for the uric acid lowering drug, Uloric (AKA Feburic and other brands).
Various Uric acid >10 for years, allergic to allopurinol, uloric safe?: One gout patient claimed indomethacin caused tinnitus, which disappeared after switching to diclofenac. But, another gout patient claimed diclofenac caused him tinnitus. Finally, the point was made that all NSAIDs can cause tinnitus.
May 2017 High Uric Acid with high blood sugar: “there is one point that keep us hesitant in increasing the dosage is because my husband is having tinnitus since starting Allopurinol. Of course all the readings & even dr. said the medicine is the not cause, but we dont know”.
That final point prompts me to offer a note of caution when we think of any side effects – not just tinnitus. Because, as humans, we always tend to connect events, even if there is no connection. So, the only way to prove it is a gout drug that is causing your tinnitus is to switch to an alternative. But, that is particularly difficult with NSAIDs. Because, all NSAIDs can cause tinnitus. Although, individuals might find that one type of NSAID is better than others.
What is your experience with tinnitus and gout drugs?
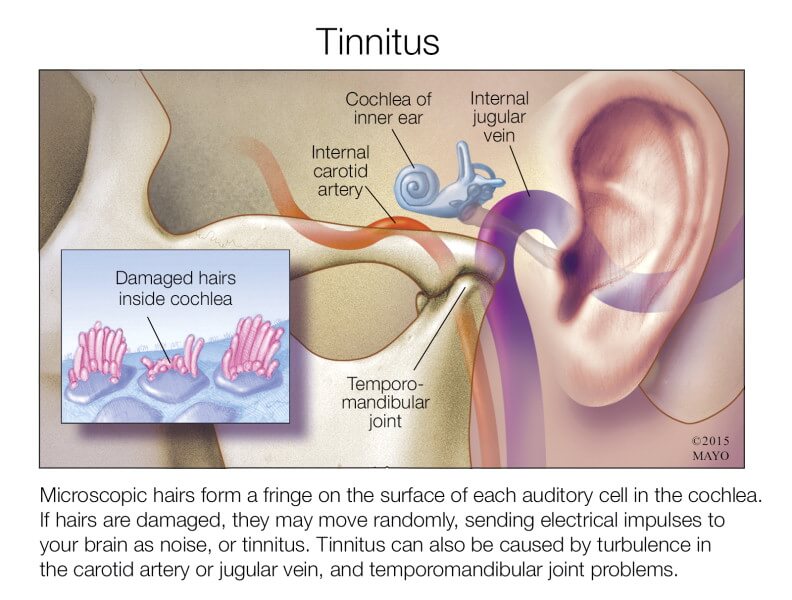
Can Gout Drugs Cause Tinnitus?
[image courtesy Mayo]Keith TaylorParticipantI’m sorry about the confusion, Marc. I must find time to document this properly.
Your choice is Casual Gout Help or Structured Gout Help. In both cases, you can ask as many questions as you like. Or share experiences and opinions.
Casual is where you just ask questions whenever you feel like it. Then, other GoutPal members and I will try to answer them. Each question is fairly isolated from others. But, you can often save repetition of facts by linking to an earlier topic.
Structured is where I create a separate forum, just for your posts. The first advantage of that is, you can create topics to record daily gout symptoms, changes to gout medicines, test results, etc. And you can organize it however you like.
Secondly, you can start to ask more complicated questions that I can answer in a step-by-step manner. It’s a form of self-paced learning, where we don’t move on to the next step until you are happy with the current step. This is great for treatment plans, or to get a more in-depth view of a particular aspect of gout.
So, Marc, the choice is yours. You tell me which you prefer. Then, I’ll explain what we do next.
Keith TaylorParticipantThanks d_q 🙂
With regard to allopurinol, I recall reading an editorial style article by a rheumatologist. Unfortunately, I can’t remember who he is, or which publication he wrote for. But, he made a case for taking allopurinol for a month each year. Ie, by taking high doses of allopurinol for a month, that should dissolve any crystals that have formed in the year. Because 11 months of crystal deposition should not be long enough to cause problems.
Of course, that is just theory for now. Also, I’m not convinced that it’s very superior to just popping a pill each day. But, it’s always good to have choices.
Keith TaylorParticipantWow, thanks for that. I’m only at the ‘ideas’ stage at the moment. So, I haven’t played with any numbers yet. But, your findings are intriguing.
I think your final paragraph goes to the heart of the problem with all food scoring systems. To the point that, I might forget the whole thing! Anyway, it isn’t my main priority at the moment. But, you’ve certainly given me food for thought. 🙂
Keith TaylorParticipantThanks for your quick response Cindy. Also, even bigger thanks to nobody for a terrific answer. Because, medically, we have established that Mr Tang is safe to proceed. But, all treatment plans have to balance risk and reward.
So, at this stage Cindy, I don’t have enough information to recommend exactly when your husband should increase his allopurinol dose. Furthermore, in an ideal world, we would not even be discussing this. Because, target uric acid levels and timescale should be discussed between patient and doctor before allopurinol therapy starts. But, in the real world, we tend to make these decisions as we go. Which is why I said in my previous reply: “The time between allopurinol dose increases is variable, depending on how quickly the doctor and patient wish to proceed”.
For example, in my case, I had a particular medical situation that supported the idea of moving forward as quickly as possible. Also, I had a supportive doctor who agreed that it would benefit me to get to maximum allopurinol dose as quickly as I could. As long as function tests raised no alarm bells.
So, as nobody advised: “tests are not the only reason to increase a dose.” Therefore, I can only repeat, I don’t know enough about your husband’s situation to decide if it’s good to increase now or later.
I hope my comments, and nobody’s, give your husband enough ideas to discuss his situation with his doctor. But, if he’s not sure what to ask, I would always suggest thinking hard about what he truly wants to achieve now. Also, think about any important events in the near future. Because, vacations, family celebrations, etc can often influence our timetable. Then, he should have enough to explain what he wants his doctor to do.
If not, I’m sure we can come up with more suggestions.
-
AuthorPosts