Krystexxa (generic name is pegloticase) has been available to gout patients in America for 2 years, and conditions of it’s license require significant safety monitoring and reporting.
This is a layman’s review of the 2012 Krystexxa safety report. You should note that there are associated changes to labeling. I will report on revised Krystexxa labels in due course.
Krystexxa Safety Report
This is a review of:
- Title:
- Long-term safety of pegloticase in chronic gout refractory to conventional treatment.
- Authors:
- Becker MA, Baraf HS, Yood RA, Dillon A, Vázquez-Mellado J, Ottery FD, Khanna D, Sundy JS
- Published:
- Ann Rheum Dis. 2012 Dec 11
Krystexxa Safety Report Introduction & Objectives
The report introduces pegloticase with some background information. I have summarized this information in my Krystexxa Introduction, so I will not repeat it here, though references are included below for completeness.
Pegloticase is a form of uricase, that was granted a licence to be sold as Krystexxa in 2010. Approval for Krystexxa was subject to ongoing safety studies. This report continues the initial 6 month Randomized Control Trials with an additional 2.5 years of study (Open Label Extension) to provide a three year review.[17]
In Open Label Extension studies, the patient knows what they are being treated with, compared to Randomized Control Trials where the patient and doctor are unaware if the treatment is placebo or medicine.
Krystexxa Safety Report Methods
Gout patients who had taken part in the Randomized Control Trials that supported the license application were eligible to take place in the Open Label Extension. They received infusions of 8 mg pegloticase every 2 or 4 weeks. Patients were monitored primarily for:
- Safety, with special interest in gout attacks and Infusion Reactions
- Side Effects (Adverse Events) evaluated and vital signs measured prior to each 2 or 4 weekly pegloticase infusion
They were also monitored for:
- Durability of pegloticase treatment responses
- Plasma Uric Acid and Serum Uric Acid measured every 12 weeks
- Serum assessed for immune reaction every 12 weeks
- Gout attacks evaluated each visit
- Tophus burden evaluated every 24 weeks by a central reader using digital photographs
Krystexxa Safety Report Results
151 gout patients entered the Open Label Extension, including 2 who had received 4 weekly pegloticase in the Randomized Control Trials but continued observation only without further treatment. A further 27 stopped treatment due to side effects, and 13 stopped treatment because the pegloticase infusion no longer reduced uric acid.
Of the total 37 months covered by the trials, patients remained in the trials for an average of 25 months, including a no-treatment observation period at the end of the trial up to 6 months.
The report includes extensive statistical analysis and observation. The important data about side effects in the 149 patients who were treated with pegloticase is:
- 106 (71%) Gout attack
- 65 (44%) Infusion Reaction
- 29 (20%) Joint pain
- 27 (18%) Upper respiratory tract infection
- 26 (17%) Pain in exremity
- 25 (17%) Back pain
- 22 (15%) Diarrhea
- 21 (14%) Peripheral edema (swelling/puffiness)
- 20 (13%) Urinary tract infection
- 17 (11%) Nausea
- 16 (11%) Headache
- 15 (10%) Fatigue
- 15 (10%) Sinusitis
- 15 (10%) Sore nose/throat
The most important aspect of the study is whether pegloticase achieves a uric acid level below 6mg/dL. Patients who did are labeled responders. Patients who failed to achieve below 6mg/dL are labeled non-reponders. The results are complicated, because responders can stop responding during the treatment. The data presented in the study is difficult to interpret absolutely, as different benefits accrue on a case-by-case basis. For example, a patient might enjoy a few weeks of rapid tophi resolution followed by a move towards no further effectiveness. 2-weekly treatment achieved better results than 4-weekly.
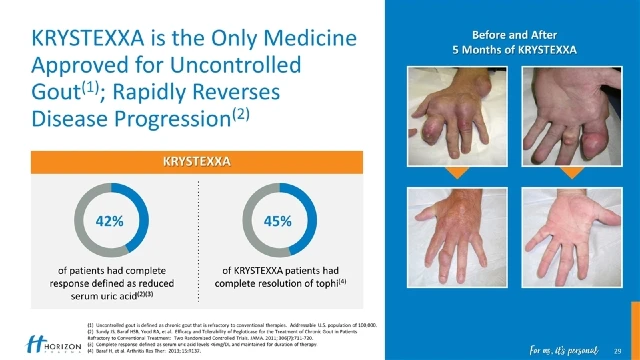
The gout patients who had visible tophi generally achieved good reduction rates. Again, various statistics across different sub-groups produce complex statistics. Each patient was assessed on up to 5 tophi, and 185 of a total 302 tophi in the study were completely resolved (61%).
The study contains information on gout attacks. As with all other types of uric acid lowering treatment, gout attacks were noticed most in the first 3 months of treatment.
Krystexxa Safety Report Discussion & Conclusion
Given that all patients had no other treatment options, long-term pegloticase was “safe and generally well tolerated”. The study showed that most Infusion Reactions occurred in patients who failed to reduce uric acid below 6mg/dL, and so it recommends that pegloticase treatment ceases if target uric acid levels are not achieved.
The authors note the general limitation of potential bias in Open Label Extension studies.[19] They also note the limitation from earlier Randomized Control Trials of separate groups of 2 weekly and 4 weekly treatment. Most patients ended with the 2 weekly treatment.
In summary, the safety profile of pegloticase in the OLE study was consistent with that observed in the RCTs [Randomized Control Trials][17] with no evidence of new safety concerns related to long-term exposure. Efficacy findings further demonstrated that clinical improvements were durable and probably progressive during long-term therapy in patients with persistent goal range urate-lowering responses to pegloticase.
Krystexxa Safety: Next Steps
If you have any questions, opinions, or experiences of Krystexxa, especially safety issues, please share them in the gout forums. Or use the feedback form below.
Leave Krystexxa Safety to browse other Krystexxa pages.
Krystexxa Safety Related Topics
Please remember: to find more related pages that are relevant to you, use the search box near the top of every page.
Common Terms: Krystexxa, pegloticase
Other posts that include these terms:
- Gout Medications To Avoid Gout By Lower Uric Acid
- Gout Treatment, Cures, Remedies & Relief
- Best Tophi Picture shows greatest Tophi Treatment
- Krystexxa (pegloticase)
- Uricase for Fast Uric Acid Control
- Advantages and Disadvantages of Uric Acid
- Treatment For Gout
Krystexxa Safety Report References
- Zhang W, Doherty M, Bardin T, et al. EULAR evidence based recommendations for gout. Part II: management. Report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis 2006;65:1312–24.
- Hamburger M, Baraf HS, Adamson TC III.et al. Recommendations for the diagnosis and management of gout and hyperuricemia. Postgrad Med 2011;123(6 Suppl 1):3–36.
- Li-Yu J, Clayburne G, Sieck M, et al. Treatment of chronic gout. Can we determine when urate stores are depleted enough to prevent attacks of gout? J Rheumatol 2001;28:577–80.
- Pascual E, Sivera F. Time required for disappearance of urate crystals from synovial fluid after successful hypouricaemic treatment relates to the duration of gout. Ann Rheum Dis 2007;66:1056–8.
- Perez-Ruiz F, Lioté F. Lowering serum uric acid levels: what is the optimal target for improving clinical outcomes in gout? Arthritis Rheum 2007;57:1324–8.
- Shoji A, Yamanaka H, Kamatani N. A retrospective study of the relationship between serum urate level and recurrent attacks of gouty arthritis: evidence for reduction of recurrent gouty arthritis with antihyperuricemic therapy. Arthritis Rheum 2004;51:321–5.
- Becker MA, Schumacher HR, MacDonald PA, et al. Clinical efficacy and safety of successful longterm urate lowering with febuxostat or allopurinol in subjects with gout. J Rheumatol 2009;36:1273–82.
- Perez-Ruiz F, Calabozo M, Pijoan JI, et al. Effect of urate-lowering therapy on the velocity of size reduction of tophi in chronic gout. Arthritis Rheum 2002;47:356–60.
- Jordan KM, Cameron JS, Snaith M, et al. British Society for Rheumatology and British Health Professionals in Rheumatology guidelines for the management of gout. Rheumatology (Oxford) 2007;46:1372–4.
- Zhu Y, Pandya BJ, Choi HK. Prevalence of gout and hyperuricemia in the US general population: the National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum 2011;63:3136–41.
- Edwards NL. Treatment-failure gout: a moving target (editorial). Arthritis Rheum 2008;58:2587–90. Treatment Failure Gout
- Brook RA, Forsythe A, Smeeding JE, et al. Chronic gout: epidemiology, disease progression, treatment and disease burden. Curr Med Res Opin 2010;26:2813–21.
- Doghramji PP, Edwards NL, McTigue J. Managing gout in the primary care setting: what you and your patients need to know. Am J Med 2010;123:S2.
- Sherman MR, Saifer MG, Perez-Ruiz F. PEG-uricase in the management of treatment-resistant gout and hyperuricemia. Adv Drug Deliv Rev 2008;60:59–68.
- Krystexxa® (pegloticase) Injection, for intravenous infusion. Prescribing information. East Brunswick, NJ: Savient Pharmaceuticals, 2010.
- Schlesinger N, Yasothan U, Kirkpatrick P. Pegloticase. Nat Rev Drug Discov 2011;10:17–18.
- Sundy JS, Baraf HS, Yood RA, et al. Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment. JAMA 2011;306:711–20.
- Richette P, Bardin T. Gout. Lancet 2010;375:318–28.
- Day RO, Williams KM. Open-label extension studies: do they provide meaningful information on the safety of new drugs? Drug Safety 2007;30:93–105.
Please give your feedback
Did this page help you? If yes, please consider a small donation. Your donations help keep GoutPal's gout support services free for everyone.
If not, please tell me how I can improve it to help you more.
- YouTube
- The gout forums.








