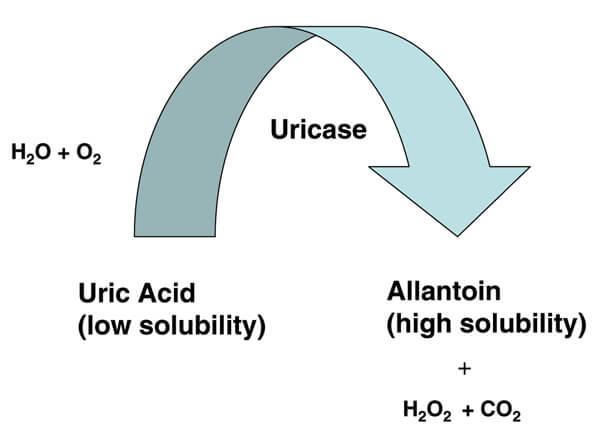
Uricase is not a gout treatment. It is an enzyme that converts uric acid to allantoin. Allantoin is much more soluble than uric acid, and passes harmlessly from the body.
Unfortunately, during evolution, humans have lost the ability to produce uricase (also called urate oxidase)[1]. Scientists will argue about the reasons for this. However, we can do nothing about the reasons, though we might be able to do something about the loss of uricase.
The Loss Of Uricase
Uricase is not totally lost to us. The bacteria that keep our digestive system working do produce uricase. However, it is not clear if this plays a part in removing uric acid from our bodies.
There is significant research in the 1950s, 1960s, and 1970s to try to understand the complex uric acid pathways[2-5]. The consensus from that research is that
Two-thirds of the uric acid is normally excreted through the kidney while one third gains entrance to the gut where it undergoes uricolysis.
Uricolysis is the process of breaking down uric acid to other compounds. Once assumed to be down to bacteria in the gut, this was discounted as early as 1953 when Wyngaarden wrote:
these results argue against the active participation of intestinal bacteria in uricolysis in man.
Given the significance of one-third of uric acid excretion not passing through the kidneys, the term extra-renal excretion was introduced to gout studies. In recent years, researchers have discovered a genetic role in extra-renal excretion[6].
Ichida and colleagues progress the identification of genetic involvement by suggesting a new way to classify gout, which could have a significant impact on future treatment. They argue that the traditional division of gout patients into over-producers and under-excreters of uric acid requires refinement.
Under excreters remains valid, but they argue that over-producers should be renamed kidney-overload (or renal overload type to use their term). Kidney-overload would then have two subgroups: genuine overproduction; and extra-renal excretion impairment.
This may seem like semantics, but it is important. Because the cause of excess uric acid can help to determine the treatment. In this case, it could influence new treatments that encourage uric acid excretion through pathways other than the kidneys.
This reminds me of a low-profile study that I saw some time ago. In September 2008, a paper was presented at the Third China-Russia International Symposium on Pharmacology titled: “Montmorillonite promotes diffusion, prevents absorption of uric acid and
decrease uric acid level in the serum.”
That research has been translated to two or three similar published articles, but I do not have access to the full text. This is in the category of “further research required,” but initial findings look promising. The paper concludes:
CONCLUSION: MMT can promote diffussion of uric acid from blood vessel to intestine, prevent absorption of uric acid in intestinal tract and decrease uric acid level in the serum.
Now, this has little to do with uricase, but it is relevant that it points to a genetic advantage indicating that we could forgo uricase because we developed other ways to excrete excess uric acid. Unfortunately, some people have a weakness with this. Montmorillonite is an untested potential remedy, but science has also developed ways to replace uricase.
Uricase Replacements
Uricase does not exist in humans, so scientists have had to prepare it from other sources. This led to the early discovery that most humans cannot tolerate uricase as a treatment. A great deal of time, effort, and money have been spent refining uricase into an acceptable treatment.
There are currently two replacement uricase products available, though neither is without problems.
Rasburicase sold as Elitek and Fasturtec
Pegloticase sold as Krystexxa
Detailed pages for these uricase-based gout treatments are coming soon. If you want to be informed when they are available, please see my Gout Info Update Service.
Although not directly uricase related, if you want to try the Montmorillonite treatment, you should discuss it with your doctor. Montmorillonite is widely available as Calcium Bentonite.
If you cannot respond to allopurinol or Uloric (febuxostat), and probenecid is only suitable for under-excreters, then Krystexxa could be good for your gout. This is best administered by a rheumatologist with experience in this new gout treatment.
Leave Uricase to browse other gout medications to avoid gout by lower uric acid.
Uricase Comments
GoutPal visitor responses and associated research include:
Uricase Medication
Gout patients in the forum have mentioned the low response rates for uricase medication. Because the antibodies that often develop during pegloticase treatment make it suitable for less than half potential candidates. But recent research indicates that uricase medication combined with an immunosuppressant yields much better results[7-8].
Uricase Related Topics
Please remember: to find more related pages that are relevant to you, use the search box near the top of every page.
Common Terms: convert, human, medication, Most Helpful Gout Pages, pegloticase, rasburicase
Other posts that include these terms:
- Krystexxa Safety
- High Alkaline Foods for Gout Diet Menu
- Gout Foods Table for Vegetables
- Gout Food List for GoutPal Foodies
- Foods High in Uric Acid Chart
- Purine Rich Foods
- Does Alcohol Affect Gout?
- Colchicine For Gout
- What Foods Cause Gout?
- Is Chinese Food Bad For Gout?
- Is Very Low Purine Gout Diet Possible?
- Edamame and Gout: Vegetable Medley
Uricase References
- Title: Loss of urate oxidase activity in hominoids and its evolutionary implications. Author(s): Oda M, Satta Y, Takenaka O, Takahata N. Published: Mol Biol Evol. 2002 May;19(5):640-53.
- Title: Uricolysis in normal man. Author(s): WYNGAARDEN JB, STETTEN D Jr. Published: J Biol Chem. 1953 Jul;203(1):9-21.
- Title: Role of the intestinal tract in the elimination of uric acid. Author(s): Sorensen L B. Published: Arthritis Rheum. 8, 694–706 (1965).
- Title: The study of human intermediary purine metabolism and its regulation. Author(s): Seegmiller J E. Published: Proc R Soc Med. 1966 April; 59(4): 292–302.
- Title: Origin and extrarenal elimination of uric acid in man. Author(s): Sorensen LB, Levinson DJ. Published: Nephron. 1975;14(1):7-20.
- Title: Decreased extra-renal urate excretion is a common cause of hyperuricemia. Author(s): Ichida K, Matsuo H, Takada T, Nakayama A, Murakami K, Shimizu T, Yamanashi Y, Kasuga H, Nakashima H, Nakamura T, Takada Y, Kawamura Y, Inoue H, Okada C, Utsumi Y, Ikebuchi Y, Ito K, Nakamura M, Shinohara Y, Hosoyamada M, Sakurai Y, Shinomiya N, Hosoya T, Suzuki H. Published: Nat Commun. 2012 Apr 3;3:764. Gout Causes: 3 Types Not 2
- Albert, John A., Tony Hosey, and Brian LaMoreaux. “Increased Efficacy and Tolerability of Pegloticase in Patients With Uncontrolled Gout Co-Treated With Methotrexate: A Retrospective Study.” Rheumatology and Therapy 7, no. 3 (2020): 639-648.
- Botson, John K., John RP Tesser, Ralph Bennett, Howard M. Kenney, Paul M. Peloso, Katie Obermeyer, Brian LaMoreaux, Michael E. Weinblatt, and Jeff Peterson. “Pegloticase in combination with methotrexate in patients with uncontrolled gout: A multicenter, open-label study (MIRROR).” The Journal of Rheumatology (2020).
Please give your feedback
Did this page help you? If yes, please consider a small donation. Your donations help keep GoutPal's gout support services free for everyone.
If not, please tell me how I can improve it to help you more.
- YouTube
- The gout forums.








